08 June 2021: Original Paper
Application of Metagenomic Next-Generation Sequencing to Diagnose Pneumonia in Kidney Transplantation Recipients
Jia Xu12345ABCDEF, Yedong Yu12345ABCD, Junhao Lv12345ABCD, Sisi Yang6ABCD, Jianyong Wu12345AD, Jianghua Chen12345AD, Wenhan Peng12345AEFG*DOI: 10.12659/AOT.931059
Ann Transplant 2021; 26:e931059






Abstract
BACKGROUND: Pneumocystis jirovecii pneumonia (PJP) is one of the common opportunistic infections diagnosed in kidney transplantation recipients. It is difficult to identify early by use of classic tools such as Grocott-Gomori stains and polymerase chain reaction (PCR). Metagenomic next-generation sequencing (mNGS) is accurate, unbiased, and sensitive, and is promising in PJP diagnosis.
MATERIAL AND METHODS: Data on kidney transplantation patients diagnosed with PJP were retrospectively analyzed. The sensitivity and specificity of different tools such as mNGS, laboratory tests, and Grocott-Gomori stains for PJP diagnosis were compared. All recipients were treated with trimethoprim-sulfamethoxazole (TMP-SMX).
RESULTS: There were a total of 12 kidney transplantation recipients diagnosed with PJP based on mNGS in our center from January 01, 2020 to October 27, 2020. Highly variable numbers of sequence reads for P. jiroveci (19 to 1041285) showed diagnostic significance. Bronchoalveolar lavage fluid (BALF) samples were tested by Grocott-Gomori staining, with only 6 of 11 (54.5%) positive. Other routine laboratory tests like routine blood tests, blood biochemistry, procalcitonin (PCT), immune function, (1,3)-β-d-glucan (BG), serum galactomannan (GM), and C-reactive protein (CRP) showed even lower efficacy. TMP-SMX appeared to be the ideal therapy for kidney transplantation recipients with PJP.
CONCLUSIONS: mNGS has utility in the diagnosis of PJP and mixed infections in kidney transplantation recipients, and TMP-SMX could be the ideal therapeutic drug for kidney transplantation recipients suffering from PJP.
Keywords: Kidney Transplantation, Metagenomics, Pneumocystis Infections, High-Throughput Nucleotide Sequencing, Pneumocystis carinii, Pneumonia, Pneumocystis
Background
Infection is one of the common complications after kidney transplantation [1–4]. Long-term use of immunosuppressants weakens both humoral and cellular immune functions. It, along with multiple changes in the postoperative physiological structures, results in pulmonary infections and urinary tract infection [1,5]. Compared with the general population, infection in kidney transplantation recipients is far more complicated and they are prone to opportunistic infections, mixed infections, rare bacterial infections, and severe infections, which makes diagnosis more difficult. Delayed diagnosis leads to delayed treatment and to poor prognosis [1,6–8]. Therefore, correct diagnosis and timely treatment are extremely important for kidney transplantation recipients with infection.
Although staining, culture, antigen detection, PCR, and other methods have been widely used in clinical practice, it is still quite difficult to quickly obtain accurate pathogen results due to the complexity of kidney recipients’ infections [9,10]. Therefore, we can only diagnose it by the recipients’ symptoms, signs, imaging examination, and laboratory examinations, and then perform empirical anti-infection treatment, which is always broad-spectrum. It comes along with many disadvantages, such as the abuse of antibiotics, the formation of multi-drug-resistant bacteria, misdiagnosis, missed diagnosis, delays in diagnosis, increased treatment costs, and even death [8,11,12]. Faster and more accurate diagnostic technology is urgently needed.
Metagenomic next-generation sequencing (mNGS) is a new diagnostic technology that can detect all pathogens in recipients’ samples quickly, accurately, and without bias, which is of great help in the identification of complex and rare pathogens [10,13,14]. With progress in the related technologies, mNGS has gradually become popular in clinical practice, especially for use in patients with severe infections, immunodeficiency, and long-term use of immunosuppressants after organ transplantation [9,13,15–17].
Material and Methods
PATIENTS AND COLLECTION OF SAMPLES:
From January 01, 2020 to October 27, 2020, there were 21 kidney transplantation recipients with symptoms of fever, dry cough, or anhelation in our center. Their CT scans suggested interstitial lung disease. Among these patients, we performed mNGS testing on patients with PO2 below 70 mmHg, and 12 of them were diagnosed as having PJP based on mNGS (1 with a sample of peripheral blood, 9 with BALF, and 2 with both). For 11 patients who underwent bronchoscopy, we performed Grocott-Gomori staining, fungus immunofluorescence staining, and other tests with their BALF. In addition, we also performed routine blood tests, blood biochemistry, PCT, immune function, (1,3)-β-d-glucan (BG), serum galactomannan (GM), procalcitonin (PCT), and C-reactive protein (CRP) on peripheral blood (PB) samples.
BALF and PB samples were obtained (about 3 mL) and placed in the sterile sputum container, stored at −20°C, then sent to REALBIO TECHNOLOGY (Shanghai, China) for detection.
MNGS PROCEDURE FOR SAMPLES:
The mNGS procedure for BALF and PB samples included sample collection, library construction, and sequencing. According to the manufacturer’s protocols, the DNA was extracted by using a TIANamp Micro DNA extraction kit and the RNA was extracted using a QIAamp Viral RNA Mini Kit RNA extraction kit. Using NanoDrop (Thermo Scientific) and Qubit®2.0 (Invitrogen, USA), the DNA/RNA concentration was measured, and the molecular size was estimated by agarose gel electrophoresis. Then, the library was constructed by using the Hieff NGS® 384 Dual Index Primers Kit for Illumina®. The quality of the library was estimated using Agilent 2100 (Agilent, USA) to estimate the concentration. Finally, the libraries constructed from all the samples were pooled and sequenced on the Illumina NextSeq platform (Illumina, San Diego, CA).
For quality control and bioinformatic analysis, we processed the raw reads of sequencing to remove low-quality reads and adapter contamination to produce clean reads. Then, we mapped the clean reads to the human-source database to filter the human-source sequence. The remaining reads were aligned to the reference database (NCBI database and GenBank) to identify microbial species.
TREATMENT:
In the past 5 years, our center has performed approximately 450 kidney transplants each year. Usually, the recipients were given basiliximab or anti-thymocyte globulin (ATG) for immunosuppression induction (7 recipients with ATG and 5 recipients with basiliximab in our study). Then, the postoperative maintenance regimens include ciclosporin (CsA)/tacrolimus, mycophenolate mofetil (MMF)/mycophenolic acid (MPA), and glucocorticoid. To prevent PJP infections, the recipients need to take TMP-SMX for 1 year after surgery. In our study, 3 recipients within 1 year after surgery did not take the prophylaxis due to their poor compliance or allograft function.
For those patients diagnosed with PJP by mNGS, we used TMP-SMX as anti-infective treatment, and regularly checked their serum creatinine.
Results
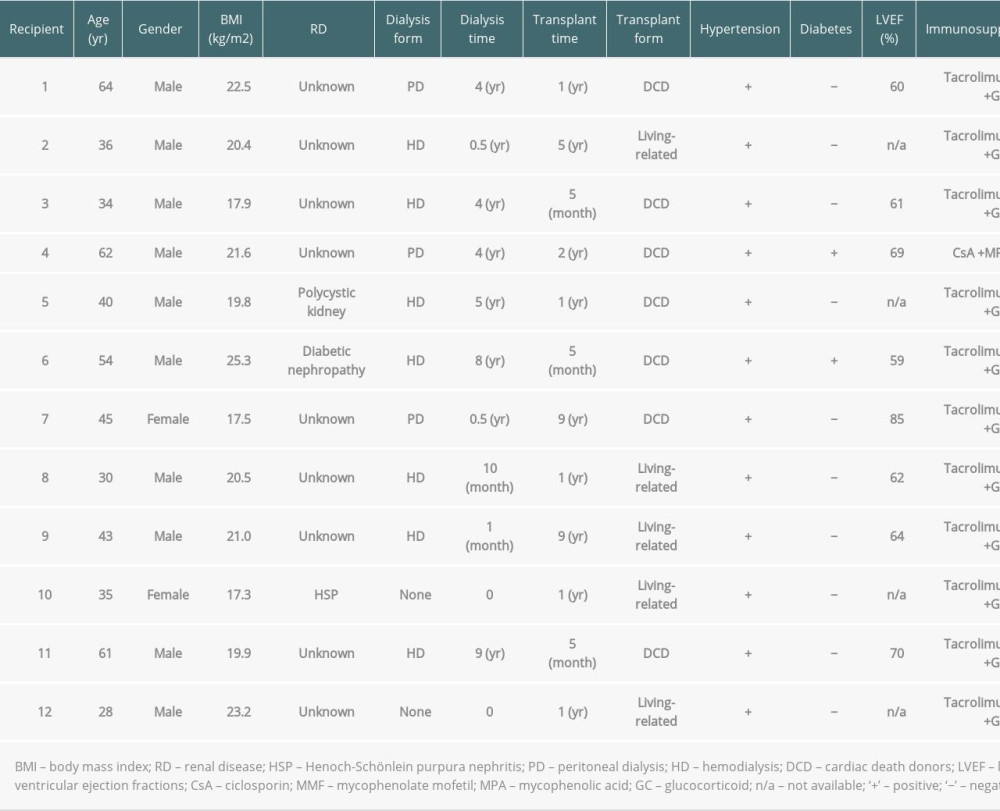
The baseline characteristics are shown in Table 1. Most recipients (83%) were male, and 70% chose hemodialysis as their form of dialysis before kidney transplantation. In addition, all of them had a history of hypertension.
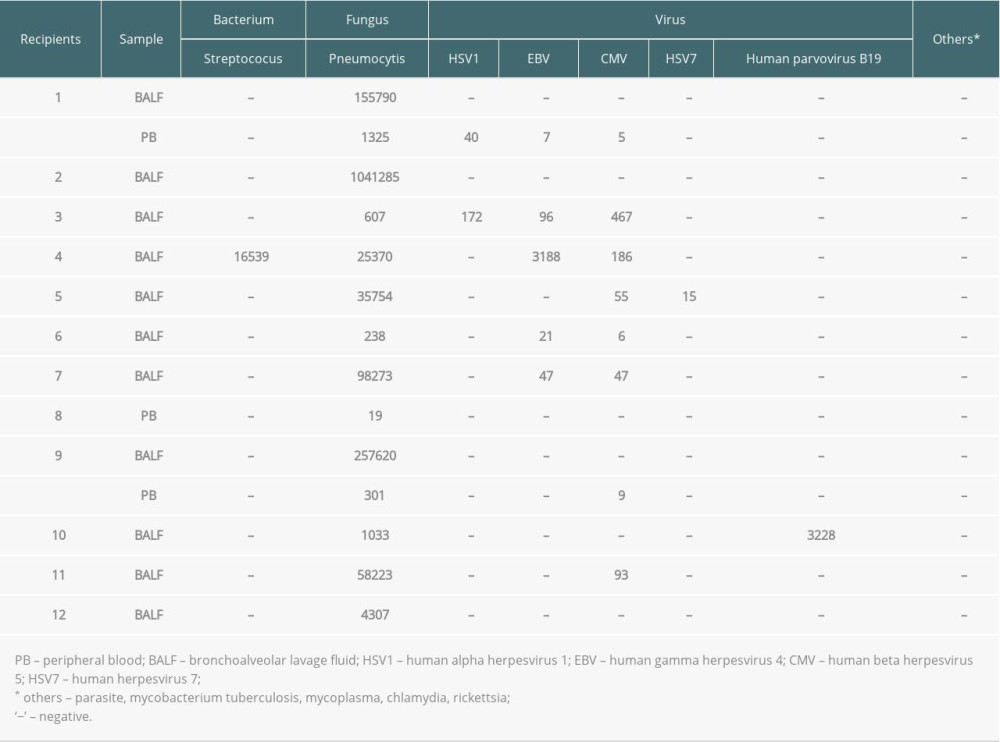
The results of mNGS are shown in Table 2. Most recipients had very high reads of pneumocystis. From the results of the 2 recipients with samples of both peripheral blood and BALF, the reads in BALF were much higher than in the peripheral blood, which may suggest that it could be more sensitive to perform mNGS with BALF than with peripheral blood. In addition, we detected some viruses such as EBV, CMV, and HSV1, so mNGS is also a great reference for the diagnosis of mixed infections. Based on the results of mNGS and laboratory tests, Recipient 4 and Recipient 10 were quickly diagnosed as having mixed infections. The pathogens of Recipient 4 were pneumocystis and streptococcus. For Recipient 10, it was pneumocystis and human parvovirus B19.
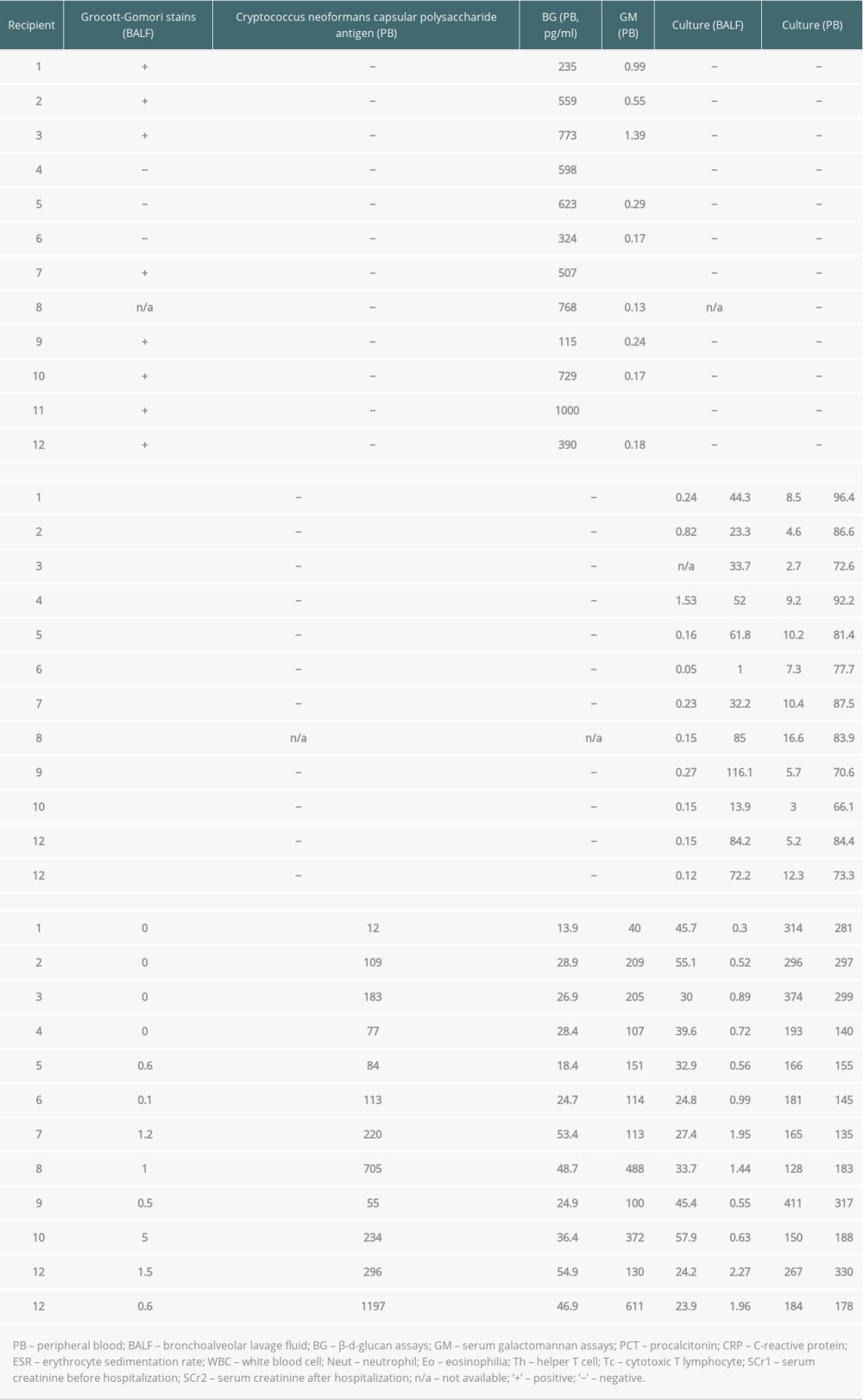
Eleven patients with BALF samples had Grocott-Gomori staining of BALF performed at the same time to find fungal asci, but only 6 patients had positive results, so the positive rate of Grocott-Gomori stains was only 54.5% in our study (Table 3). We performed a series of laboratory tests on these 12 patients (Table 3), and their BG were all positive. In addition, for 11 recipients with samples of BALF, we performed cultures for
Twelve patients diagnosed with PJP by mNGS were administered TMP-SMX as anti-infective treatment, while 2 co-infected patients were given other anti-infective drugs based on mNGS, and another 10 patients were given TMP-SMX only. Among them, 11 patients gradually recovered and were discharged, and 1 patient (Recipient 1) was transferred to the ICU for further treatment because of uncontrollable pulmonary infections (he was co-infected with human parvovirus during hospitalization). It is worth mentioning that for Recipient 10, with mixed infections, we used TMP-SMX combined with human gammaglobulin (20 g daily for 5 days); her hemoglobin increased progressively and her pulmonary infection recovered gradually.
Since the use of TMP-SMX may cause damage to renal function, we regularly checked the serum creatinine levels (Table 3). Comparing their serum creatinine at the time of admission and discharge, we found that 3 patients had relatively significant increases (>10%) in serum creatinine.
Discussion
In summary, typical symptoms, typical chest CT images, and positive BG results could be hints for the diagnosis of PJP, but these often lack specificity; interstitial pneumonia caused by other pathogens such as Cryptococcus can also have the above manifestations. At the same time, the sensitivity of Grocott-Gomori stains is inadequate [25], which may cause missed diagnosis, and many patients may not able to tolerate bronchoscopy or alveolar lavage. In addition, since dry cough is a typical symptom, sputum is not obtained in many patients for Grocott-Gomori staining. In addition, PCR testing is fast and sensitive, but it relies on certain assumptions and has not been approved for the clinical diagnosis of PJP in some countries, such as the United States and China. Therefore, mNGS has great significance in the diagnosis of PJP and mixed infections in kidney transplantation recipients. It does not require making assumptions about pathogens, and is sensitive to bacteria, viruses, fungi, and parasites, with no bias [13,14,26,27].
The sequence reads for
mNGS can help clinicians make rapid diagnosis, provide early treatment and timely intervention, and speed the clinical decision-making of antibiotic treatment programs, thereby promoting early recovery of the recipients and reducing hospitalization time and economic expenditure. In addition, it can greatly ease the abuse of antibiotics, which will have extremely important value for our entire society [12,14].
In the process of using mNGS to assist clinical diagnosis, there are some shortcomings. For example, the cost of mNGS is still relatively high [9,14]. However, the use of mNGS is helpful for early diagnosis of pathogens, thereby avoiding a series of unnecessary examinations and treatments, and the patient’s course of disease and hospital stay will be greatly reduced. Taken together, the patient’s cost may be reduced. In addition, the routine use of TMP-SMX after transplantation, coupled with the low popularity of mNGS, resulted in the small sample size of this study. However, as more and more researchers and clinicians realize the utility of this technology, we may be able to conduct a series of studies with larger sample size.
We have also observed that the timely use of TMP-SMX after the diagnosis of PJP had very good effects; the mortality rate in our center is about 8%, which is lower than the 10% reported in other studies [23]]. However, TMP-SMX can damage renal function; therefore, it is very important to select the appropriate dose and course of treatment, and to monitor renal function.
Conclusions
Our clinical experience in using mNGS shows that mNGS has utility for the diagnosis of PJP and mixed infections in kidney transplantation recipients.
References
1. Patel R, Paya CV, Infections in solid-organ transplant recipients: Clin Microbiol Rev, 1997; 10(1); 86-124
2. Sayegh MH, Carpenter CB, Transplantation 50 years later – progress, challenges, and promises: N Engl J Med, 2004; 351(26); 2761-66
3. Svobodová I, Honsová EInfections after kidney transplantation: Cesk Patol, 2015; 51(3); 120-22 [in Czech]
4. Ponticelli C, Tarantino A, Vegeto A, Renal transplantation, past, present and future: J Nephrol, 1999; 12(Suppl 2); S105-10
5. Fishman JA, Infection in solid-organ transplant recipients: N Engl J Med, 2007; 357(25); 2601-14
6. Abbott KC, Oliver JD, Hypolite I, Hospitalizations for bacterial septicemia after renal transplantation in the united states: Am J Nephrol, 2001; 21(2); 120-27
7. Fishman JA, Infection in Organ Transplantation: Am J Transplant, 2017; 17(4); 856-79
8. Pourmand G, Salem S, Mehrsai A, Infectious complications after kidney transplantation: A single-center experience: Transpl Infect Dis, 2007; 9(4); 302-9
9. Graf EH, Simmon KE, Tardif KD, Unbiased detection of respiratory viruses by use of RNA sequencing-based metagenomics: A systematic comparison to a commercial PCR panel: J Clin Microbiol, 2016; 54(4); 1000-7
10. Young BA, Hanson KE, Gomez CA, Molecular diagnostic advances in transplant infectious diseases: Curr Infect Dis Rep, 2019; 21(12); 52
11. Kollef KE, Schramm GE, Wills AR, Predictors of 30-day mortality and hospital costs in patients with ventilator-associated pneumonia attributed to potentially antibiotic-resistant gram-negative bacteria: Chest, 2008; 134(2); 281-87
12. Aryee A, Price N, Antimicrobial stewardship – can we afford to do without it?: Br J Clin Pharmacol, 2015; 79(2); 173-81
13. Simner PJ, Miller S, Carroll KC, Understanding the promises and hurdles of metagenomic next-generation sequencing as a diagnostic tool for infectious diseases: Clin Infect Dis, 2018; 66(5); 778-88
14. Goldberg B, Sichtig H, Geyer C, Making the leap from research laboratory to clinic: Challenges and opportunities for next-generation sequencing in infectious disease diagnostics: mBio, 2015; 6(6); e01888-15
15. Swaminathan S, Schlaberg R, Lewis J, Fatal Zika virus infection with secondary nonsexual transmission: N Engl J Med, 2016; 375(19); 1907-9
16. Fischer N, Indenbirken D, Meyer T, Evaluation of unbiased next-generation sequencing of RNA (RNA-seq) as a diagnostic method in influenza virus-positive respiratory samples: J Clin Microbiol, 2015; 53(7); 2238-50
17. Wilson MR, Naccache SN, Samayoa E, Actionable diagnosis of neuroleptospirosis by next-generation sequencing: N Engl J Med, 2014; 370(25); 2408-17
18. Thomas CF, Limper AH, Pneumocystis pneumonia: N Engl J Med, 2004; 350(24); 2487-98
19. Kovacs JA, Hiemenz JW, Macher AM: Ann Intern Med, 1984; 100(5); 663-71
20. Yale SH, Limper AH: Mayo Clin Proc, 1996; 71(1); 5-13
21. Mu XD, Jia P, Gao L, Relationship between radiological stages and prognoses of pneumocystis pneumonia in non-AIDS immunocompromised patients: Chin Med J (Engl), 2016; 129(17); 2020-25
22. Winston DJ, Lau WK, Gale RP, Young LS: Ann Intern Med, 1980; 92(6); 762-69
23. Sepkowitz KA, Opportunistic infections in patients with and patients without Acquired Immunodeficiency Syndrome: Clin Infect Dis, 2002; 34(8); 1098-107
24. Procop GW, Haddad S, Quinn J: J Clin Microbiol, 2004; 42(7); 3333-35
25. Chen J, He T, Li X: Infect Drug Resist, 2020; 13; 2829-36
26. Naccache SN, Federman S, Veeraraghavan N, A cloud-compatible bioinformatics pipeline for ultrarapid pathogen identification from next-generation sequencing of clinical samples: Genome Res, 2014; 24(7); 1180-92
27. Chiu CY, Viral pathogen discovery: Curr Opin Microbiol, 2013; 16(4); 468-78
In Press
18 Mar 2024 : Original article
Does Antibiotic Use Increase the Risk of Post-Transplantation Diabetes Mellitus? A Retrospective Study of R...Ann Transplant In Press; DOI: 10.12659/AOT.943282
20 Mar 2024 : Original article
Transplant Nephrectomy: A Comparative Study of Timing and Techniques in a Single InstitutionAnn Transplant In Press; DOI: 10.12659/AOT.942252
28 Mar 2024 : Original article
Association Between FEV₁ Decline Rate and Mortality in Long-Term Follow-Up of a 21-Patient Pilot Clinical T...Ann Transplant In Press; DOI: 10.12659/AOT.942823
02 Apr 2024 : Original article
Liver Transplantation from Brain-Dead Donors with Hepatitis B or C in South Korea: A 2014-2020 Korean Organ...Ann Transplant In Press; DOI: 10.12659/AOT.943588
Most Viewed Current Articles
05 Apr 2022 : Original article
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
12 Jan 2022 : Original article
Risk Factors for Developing BK Virus-Associated Nephropathy: A Single-Center Retrospective Cohort Study of ...DOI :10.12659/AOT.934738
Ann Transplant 2022; 27:e934738
22 Nov 2022 : Original article
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988
15 Mar 2022 : Case report
Combined Liver, Pancreas-Duodenum, and Kidney Transplantation for Patients with Hepatitis B Cirrhosis, Urem...DOI :10.12659/AOT.935860
Ann Transplant 2022; 27:e935860