15 June 2022: Human Study
Evaluation of Apical Leakage After Root Canal Obturation with Glass Ionomer, Resin, and Zinc Oxide Eugenol Sealers Combined with Thermafil
Violeta VulaDOI: 10.12659/MSMBR.936675
Med Sci Monit Basic Res 2022; 28:e936675






Abstract
BACKGROUND: A hermetic seal at the apical terminus is required for healthy periradicular tissue. Root canal obturation sealers that are used in endodontics are based on zinc oxide eugenol, calcium hydroxide, resins, glass ionomers, silicone, or bioceramics, but no optimal sealer material has been identified to date. Therefore, the aim of this in vitro study was to evaluate apical leakage after crown-down preparation and root canal obturation with Endomethasone N, glass ionomer cement, and EndoRez sealers.
MATERIAL AND METHODS: For this in vitro study, we tested 92 extracted human teeth, which were divided into 3 groups after a preparation technique and obturation with Endomethasone N sealer, glass ionomer cement, and EndoRez sealer in combination with Thermafil obturator. Apical leakage was evaluated and compared among the tested groups using a dye leakage method through a stereomicroscope. The values were measured from the apex to the coronal extent of dye penetration. For statistical analysis, the t test was used for comparison of the arithmetic averages of tested groups.
RESULTS: After preparation with rotary files, tested groups obturated with Thermafil obturator in combination with Endomethasone sealer showed higher average dye penetration than tested groups obturated with EndoRez and glass ionomer sealer.
CONCLUSIONS: Although all experimental groups showed dye leakage, the glass ionomer sealer in combination with Thermafil showed the least leakage, compared with EndoRez and Endomethason N.
Keywords: Dental Leakage, Root Canal Filling Materials, Root Canal Obturation, Acrylic Resins, Epoxy Resins, Eugenol, Glass Ionomer Cements, Gutta-Percha, Humans, Silicon Dioxide, Zinc Oxide
Background
Successful endodontic treatment is the result of adequate root canal shaping and cleaning and hermetic coronal and apical sealing [1]. The objective of endodontic treatment is infection elimination and prevention of microbial invasion in the periapical region [2]. Mechanical root canal instrumentation, an important phase of root canal treatment that also presents difficult practical challenges, must be combined with irrigation to ensure effective shaping and cleaning of the root canal system [3]. For many years, root canals were instrumented with stainless steel files or reamers using a step-back or incremental technique [4,5]. However, this method was shown to be difficult to complete, with sharp-ended instruments using a push-pull filing motion [6]. Problems encountered with this method include blockage of the root canal with debris, difficulties with irrigant penetration, procedural errors such as canal transportation and ledge formation, and the time-consuming nature of the task [7]. The limitations of this technique led to the development of the more advanced crown-down technique, which ensures adequate irrigation penetration, minimizes coronal flute binding of files, reduces straightening of the root canal after instrumentation, and ensures the extrusion of debris coronally, which prevents inoculation of microbes into the periradicular tissue [6,8,9]. The crown-down technique is currently the preferred approach to canal preparation, and it uses a variety of advanced instruments. Shaping and cleaning of the root canal system are followed by 3D obturation of the root canal.
Obturation techniques require endodontic sealers and core materials, commonly gutta-percha. Gutta-percha fills most of the endodontic space in combination with an endodontic sealer. The sealer fills the space between the gutta-percha and the root canal walls, as well as irregularities in the root canal wall and the dentinal tubules [10,11].
Endodontic sealers with antimicrobial activity can destroy residual microorganisms in the root canals [12] in combination with cold lateral or warm vertical gutta-percha condensation techniques. Thermoplasticized gutta-percha techniques showed better outcomes than did cold lateral condensation [13].The warm vertical gutta-percha condensation technique enables better adaptation and homogeneous root canal sealing but can cause extrusion of material into the periapical region and take time for realization. Among some warm gutta-percha condensation techniques, the Thermafil system technique take less time for root canal obturation, with promising results [14]. Factors such as operator’s experience, additional training in endodontics, and working situation influenced the obturation technique choice [15].
Sealers are classified according to their chemical ingredients: resin, zinc oxide eugenol (ZOE), mineral trioxide aggregate, bio-ceramic, glass ionomer, and calcium hydroxide containing sealers. Resin-containing sealers exhibit excellent physical properties, effective bonding between gutta-percha and the root canal walls, and an ability to form an apical seal with providing resistance to leakage [2,16]. Zinc oxide sealers can be eugenol or non-eugenol based, but zinc oxide is the main component of these sealers. Some ZOE sealers contain medicated agents such as paraformaldehyde, corticosteroids, or heavy metals. Endomethasone N is a modification of an endomethasone sealer that does not contain paraformaldehyde [17]. Glass ionomer cement (GIC) has a bacteriostatic action on account of the fluorides it contains. Fluoride released into the root canal by the GIC acts bacteriostatically on the microorganisms remaining in the dentin tubules and those coming from micro-spaces [18,19]. Despite the availability of various endodontic sealers and root canal obturation techniques, endodontic failure can still occur. Apical micro-leakage can appear due to the physical and chemical properties of the sealers or the root canal preparation and obturation techniques [20]. Microleakage can be due to differences in the thermal coefficient of expansion of the material and the tooth tissue, the presence of a smear layer, the consistency and quantity of the endodontic sealer, the solubility of the material, or the inadequacy of the obturation [21]. The presence of micro-spaces allows the penetration of tissue fluids into the root canal system. This transudate, which flows continuously into the canal, originates from the blood serum. The serum undergoes degradation and diffuses into the periradicular tissue. This serum with the remaining bacteria and their endotoxins initiate periradicular inflammation and microleakage [22]. To date, various in vitro methodologies were used for evaluation of endodontic material properties, generally by measuring microleakage, which allows an agent in trace to penetrate the filled root canal. Commonly used tracers are dyes, radioisotopes, bacteria, and their endotoxin products [23–25].
This study aimed to evaluate and compare apical sealing in root canals filled with gutta-percha and the root canal sealers Endomethasone N (Septodont, Saint Maur des Fosses, France), EndoRez (Ultradent Products, South Jordan, UT, USA), and GIC Fuji I (GC Corporation, Tokyo, Japan) after root canal instrumentation with a crown-down technique.
Material and Methods
Ethics commission approval (no. 269/2014) was given from the Faculty of Medicine in the University of Prishtina. A total of 92 human upper central incisors that had fully formed apices and had been extracted for periodontal reasons were included in this study. The approval from the patients had been taken for the use of their non-restorable teeth.
The teeth were preserved in normal saline after extraction. On the first day of the experiment, the teeth were immersed for 2 h in 1% sodium hypochlorite. The water-cooled diamond disk served to remove the tooth crown at the cement-enamel junction. The root canal patency was checked and the root canal working length was determined with a no. 15 K-file (Dentsply Maillefer, Ballaigues, Switzerland) until the tip was visible at the apical foramen and was then brought back 1 mm. Then root canal working length was measured using the endodontic ruler and was confirmed by radiographic X-rays. The root canal working length was not unified for all samples. The root canals were divided into 3 experimental groups according to the sealers used. All 3 tested groups were prepared with the ProTaper rotary system (Dentsply Maillefer) according to the manufacturer’s instructions. The root canals were disinfected with sodium hypochlorite after each file was used. The coronal third of the root canal was prepared with SX files, then the middle and apical thirds were instrumented with shaping files S1 and S2 and finished with F1, F2, and F3 files to the working length of the root canal. Thus, apical preparation was completed to a size of 30. The root canals were prepared with an X-Smart endodontic motor (Dentsply Maillefer) at 300 rpm and irrigated with sodium hypochlorite after each file was used. The first group of samples (n=20) after crown-down preparation were filled with Endomethasone N sealer in combination with warm gutta-percha and Thermafil obturator. The second group of samples (n=20) were filled with EndoRez sealer, and the third group of samples (n=20) were filled with GIC in combination with Thermafil obturator. Before obturation, a Thermafil obturator was inserted into the root canal for verification. To prevent the risk of overfilling beyond the apex, 1 mm was cut off at the tip. After sealer application, the Thermafil obturator was heated in a Thermaprep Plus oven for 15 s and inserted to the root canal working length.
Cavit (3M ESPE, Seefeld, Germany) was placed as a temporary filling. The samples were stored in an incubator at 37°C under conditions of absolute humidity for a period of 7 days. Nail varnish was used to coat the surface of the roots with 2 layers. The apical sector of the experimental groups (2 mm) was left uncoated. The samples of the positive control group (n=16) were filled with Thermafil obturator without paste and left uncoated with nail polish. The samples of the negative control group (n=16) were filled with Thermafil obturator and paste and then fully coated with nail varnish. A dye penetration test was used to measure apical microleakage. The samples were placed in 2% methylene blue solution for 2 days, washed under water, and dried. After longitudinally sectioning the root in a vertically direction with a diamond disk, apical leakage was measured from the apex to the coronal direction point of the methylene blue dye penetration. Methylene blue apical leakage was recorded with a stereomicroscope (Brunel Microscope MX6T, Wiltshire, UK) at ×20 and ×30 magnification (Figure 1A–1C). All samples were examined twice in each magnification. Data were statistically analyzed through descriptive analysis to determine the arithmetic mean, standard deviation, standard error, and confidence interval with 95% reliability (95% CI). The
Results
The negative control group samples that were filled with Thermafil obturator and paste and fully coated with nail varnish showed no dye leakage. In contrast, the samples of the positive control group that were filled with Thermafil obturator but not coated with nail varnish showed dye leakage (Figure 2A, 2B).
Table 1 presents the means and standard deviations for dye leakage of sealers in the experimental groups that were sealed with Endomethasone N, EndoRez, and GIC in combination with Thermafil obturator. The mean value of dye leakage was 0.16 mm in the samples that were sealed with Endomethasone N paste in combination with Thermafil obturator. The mean value of dye leakage was 0.07 mm in the EndoRez group and 0.01 mm in the GIC group (Figures 3–5).
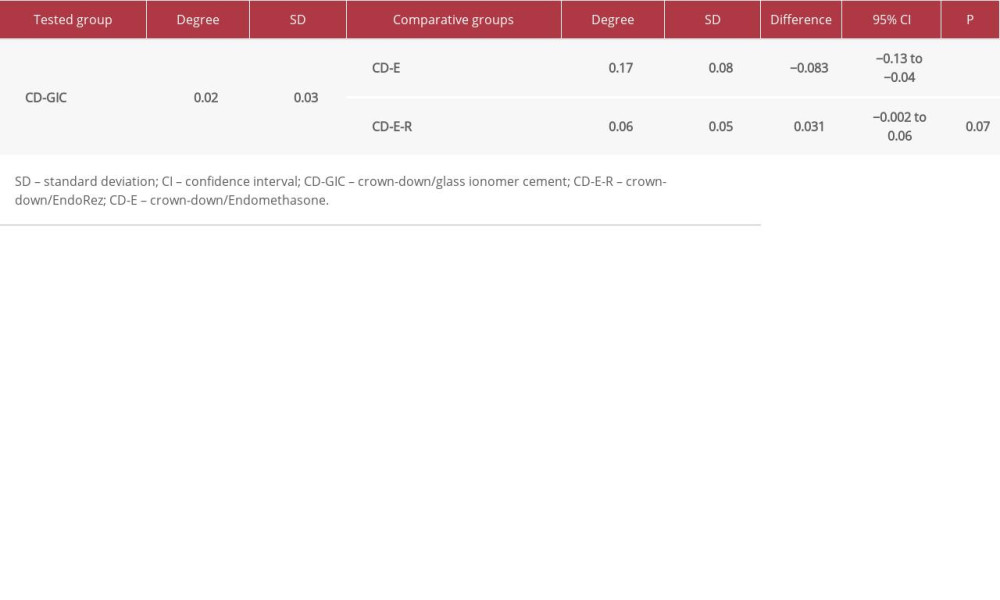
Table 2 shows the differences in the average values for dye leakage in the 3 experimental groups. The Endomethasone N group showed a greater difference in average dye leakage than GIC sealer after obturation with warm gutta-percha (average difference=−0.083mm, 95% CI −0.13 to −0.04 mm,
Discussion
The absence of microleakage contributes to successful root canal treatment. Therefore, adequate sealing by the root canal sealer is required to entomb persistent microorganisms remaining in the dentine tubules or in the complex root canal anatomy and those that are not removed by the mechanical and chemical preparation [26]. Although no current sealers effectively seal the entire root canal system, many investigators have used microleakage studies with dye penetration to try to find the best sealers that do not shrink after root canal treatment [1,27]. Dye microleakage investigations are studies that are commonly used to evaluate the sealing ability of a root canal sealer. Methylene blue dye was used in our study due to its similar or lower molecular weight, compared with that of bacterial toxins [28].
A Thermafil obturation system was used in this study, since it was shown that core-carrier obturators produce a higher gutta-percha/sealer ratio, which leads to less apical leakage [29]. In our study, in which samples were instrumented with a crown-down technique and obturated with a Thermafil obturator in combination with GIC, EndoRez, and Endomethasone N sealer, we found that the maximal level of dye leakage was 0.09 mm for GIC, 0.13 mm for EndoRez, and 0.23 mm for Endomethasone N.
Similar to our findings, Friedman et al [30] found that GIC endodontic sealers produced good results that supported their clinical use in endodontic therapy. McDougall et al [31] found that a GIC-based sealer exhibited good sealing ability which prevented the penetration of
In the present study, EndoRez provided better apical adaptation when compared with Endomethasone N paste because it showed less dye leakage. This may be attributed to EndoRez being an epoxy resin-based sealer with good physical properties, including a long setting time, low solubility, high flow rate, low volumetric polymerization shrinkage, and interfacial adaptation [36,37]. Additionally, studies have reported that EndoRez can effectively seal the root canal in combination with cold and warm gutta-percha owing to the hydrophilic properties of EndoRez, which ensure that the sealer penetrates the moist dentin and dentinal tubules [38] and provides stronger bonding capacity [39].
Similar to our results, Patni et al [40] found that ZOE sealers exhibited more microleakage than resin sealers, while Jeanneau et al [41] and Teixeira et al [42] reported satisfactory results of Endomethasone N sealer in several aspects when evaluated.
The capacity of glass ionomer to bond to dentine may be the reason our results are in concordance with those of Gargi et al [43], who also found that ZOE paste showed more microleakage than GIC. Since microleakage methods are different, the need for the standardization of microleakage detection increases in order to achieve clinically relevant results.
The differences in the results of comparing sealers between investigations, including our study, might be due to differences in experimental conditions. Therefore, further investigations are needed to evaluate the sealing ability of the materials tested in our study and other root canal sealers.
Conclusions
The results of our study have shown that all 3 root canal sealers in combination with a Thermafil obturator after crown-down preparation showed dye leakage, that GIC in combination with a Thermafil obturator showed less leakage than EndoRez sealer, and that Endomethasone N sealer showed the most dye penetration in the root canal, compared with GIC and EndoRez.
Figures
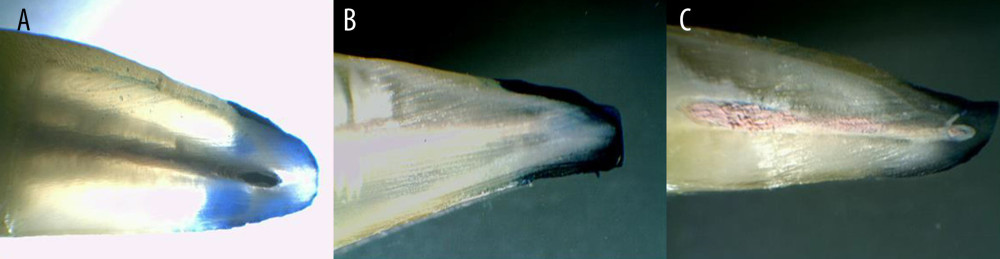 Figure 1. (A) Apical dye leakage after filling with Endomethasone N paste and Thermafil obturator. (B) Apical dye leakage after filling with EndoRez paste and Thermafil obturator. (C) Apical dye leakage after filling with GI sealer and Thermafil obturator.
Figure 1. (A) Apical dye leakage after filling with Endomethasone N paste and Thermafil obturator. (B) Apical dye leakage after filling with EndoRez paste and Thermafil obturator. (C) Apical dye leakage after filling with GI sealer and Thermafil obturator. 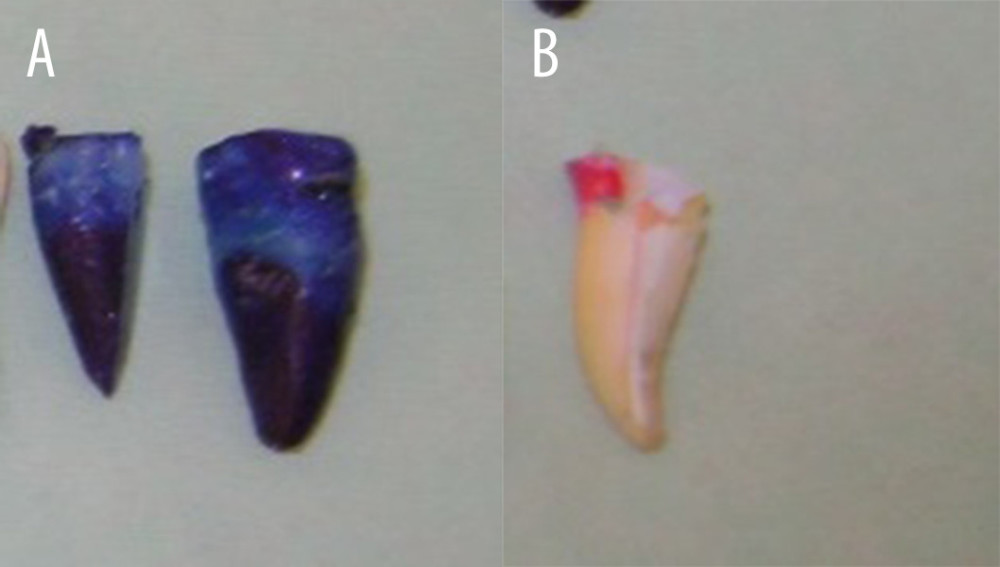 Figure 2. (A) Dye leakage in positive control group. (B) Apical dye leakage in negative control group.
Figure 2. (A) Dye leakage in positive control group. (B) Apical dye leakage in negative control group. 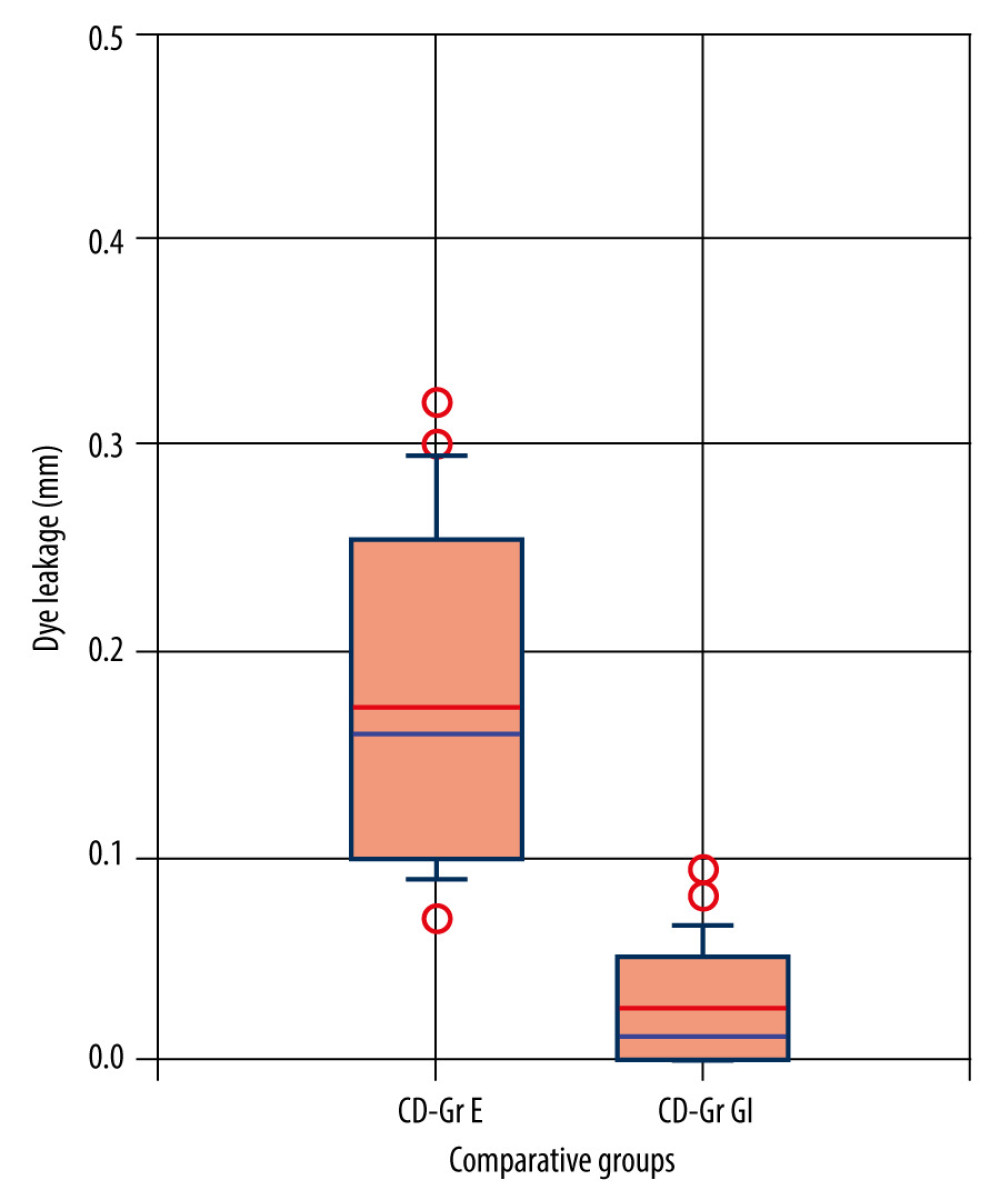 Figure 3. Dye leakage level comparation between Endomethasone and GI cement tested groups.
Figure 3. Dye leakage level comparation between Endomethasone and GI cement tested groups. 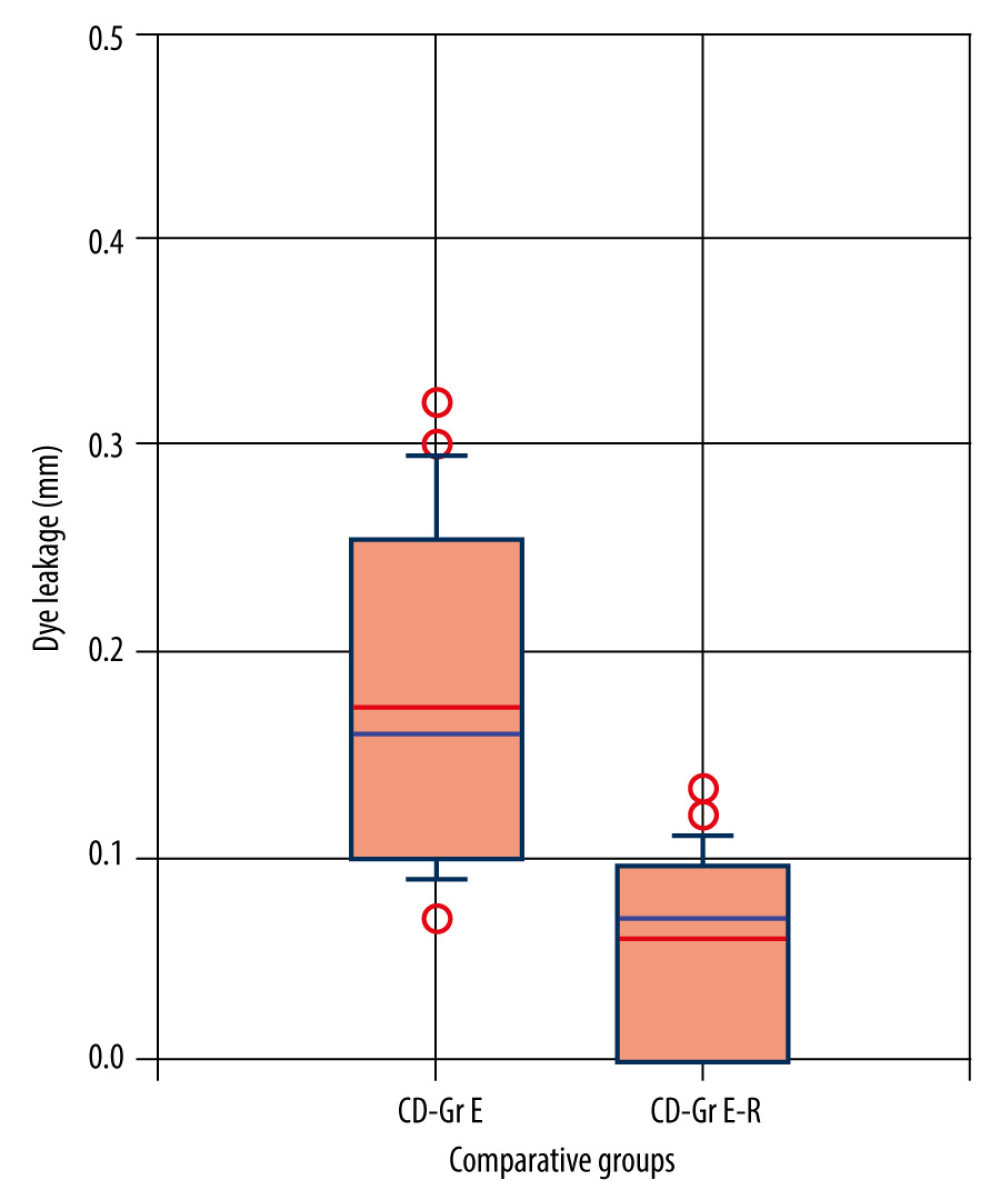 Figure 4. Dye leakage level comparation between Endomethasone and EndoRez tested groups.
Figure 4. Dye leakage level comparation between Endomethasone and EndoRez tested groups. 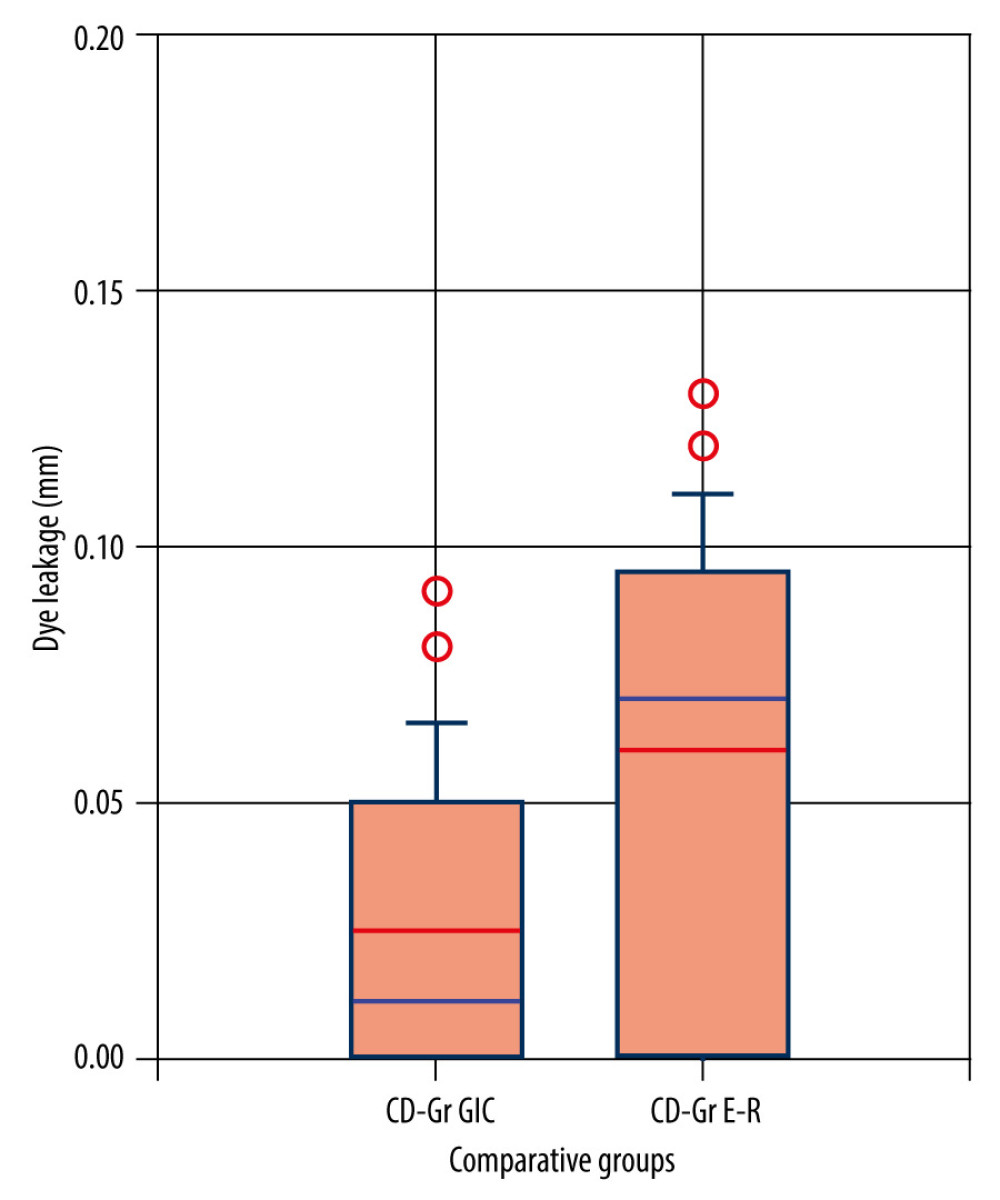 Figure 5. Dye leakage level comparation between glass ionomer cement and EndoRez tested groups.
Figure 5. Dye leakage level comparation between glass ionomer cement and EndoRez tested groups. 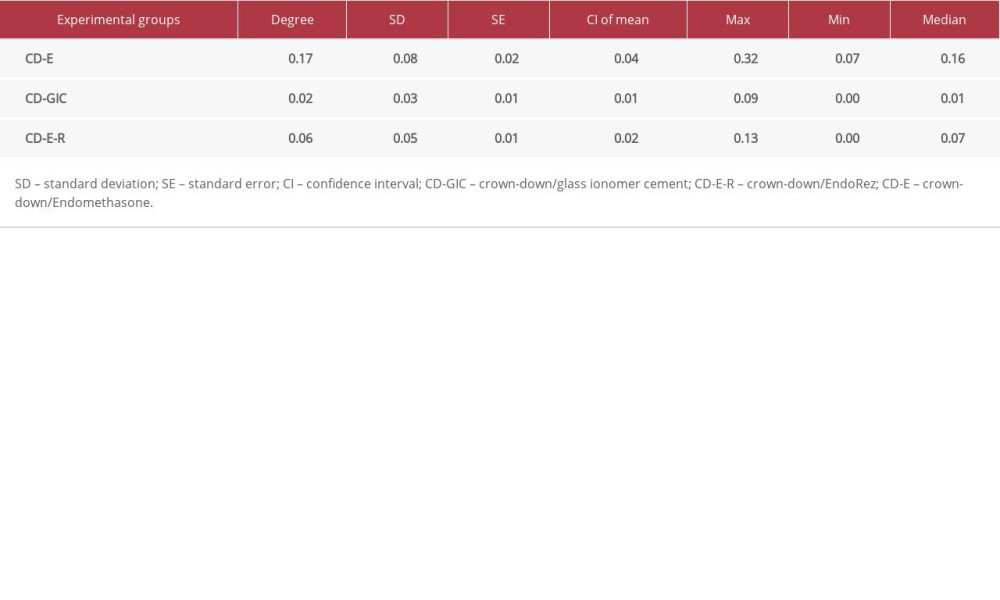
References
1. Muliyar S, Shameem KA, Thankachan RP, Microleakage in endodontics: J Int Oral Health, 2014; 6(6); 99-104
2. Rathi CH, Chandak M, Nikhade P, Functions of root canal sealers – a review: J Evolution Med Dent Sci, 2020; 9(17); 1454-58
3. Tomson PL, Simon SR, Contemporary cleaning and shaping of the root canal system: Prim Dent J, 2016; 5(2); 46-53
4. Clem W, Endodontics in the adolescent patient: Dent Clin North Am, 1969; 13(2); 483-86
5. Weine F, Healeey L, Gerstein H, Evanson L, Pre-curved files and incremental instrumentation for root canal enlargement: J Can Dent Assoc, 1970; 36(4); 155-57
6. Waplington M, McRobert AS, Shaping the root canal system: Brit Dent J, 2014; 216(6); 293-97
7. Oikonomou I, Spanaki-Voreadi A, Georgopoulou M, Procedural errors during root canal treatment performed by undergraduate students in Athens: A prospective study: Int Endod J, 2007; 40(12); 982
8. Hülsmann M, Peters O, Dummer P, Mechanical preparation of root canals: Shaping goals, techniques and means: Endod Topics, 2005; 10(1); 30-76
9. Morgan LF, Montgomery S, An evaluation of the crown-down pressureless technique: J Endod, 1984; 10(10); 491-98
10. Balguerie E, Van Der Sluis L, Vallaeys K, Sealer penetration and adaptation in the dentinal tubules: A scanning electron microscopic study: J Endod, 2011; 37(11); 1576-79
11. Ingle JI: Ingle’s endodontics, 2008, Connecticut, Pmph USA Ltd
12. Alzaidy FA, Khalifa AK, Emera RM, The antimicrobial efficacy of nanosilver modified root canal sealer: EJRMS, 2018; 6(4); 324-33
13. Bhandi S, Mashyakhy M, Abumelha AS, Complete obturation-cold lateral condensation vs. thermoplastic techniques: A systematic review of micro-CT studies: Materials (Basel), 2021; 14(14); 4013
14. Peng L, Ye L, Tan H, Zhou X, Outcome of root canal obturation by warm Gutta-Percha versus cold lateral condensation: A meta-analysis: J Endod, 2007; 33; 106-9
15. Vasconcelos I, António Ginjeira C, A survey on root canal obturation trends: Warm versus cold obturation technique: Giornale Italiano di Endodonzia, 2021; 35; 151-62
16. Kumar NS, Palanivelu A, Narayanan LL, Evaluation of the apical sealing ability and adaptation to the dentin of two resin-based Sealers: An in vitro study: J Conserv Dent, 2013; 16(5); 449-53
17. Ayer A, Manandhar TR, Agrawal N, A comparative study of apical microleakage of different root canal sealers by apical dye penetration: Bangla J Med Sci, 2017; 16(2); 219-24
18. Mohammadi Z, Shalavi S, Clinical applications of glass ionomers in endodontics: A review: Int Dent J, 2012; 62(5); 244-50
19. Saunders WP, Saunders EM, Herd D, The use of glass-ionomer as a root sealer-pilot study: Int Endod J, 1992; 25(5); 238-44
20. El Sayed MA, Taleb AA, Balbahaith MS, Sealing ability of three single-cone obturation systems: An in-vitro glucose leakage study: J Conserv Dent, 2013; 16(6); 489-93
21. Miletić I, Ribarić SP, Karlović Z, Apical leakage of five root canal sealers after one year of storage: J Endod, 2002; 28(6); 431-32
22. Pitts D, Williams B, Morton TH, Investigation of the role of endotoxin in periapical inflammation: J Endod, 1982; 8(1); 10-18
23. Fraunhofer JA, Fagundes DK, McDonald NJ, Dumsha TC, The effect of root canal preparation on microleakage within endodontically treated teeth: An in vitro study: Int Endod J, 2000; 33(4); 355-60
24. Carratu P, Amato M, Riccitiello F, Rengo S, Evaluation of leakage of bacteria and endotoxins in teeth treated endodontically by two different techniques: J Endod, 2002; 28(4); 272-75
25. Milani AS, Firuzi S, Barhaghi MH, Evaluation of sealing abilitiy of mineral trioxide aggregate mixed with propylene glycol as a root canal sealer: A in vitro study: Dent Res J, 2019; 16(4); 216-20
26. Sreedev C, Raju I, Kumaravadivel K, Influence of different types of root canal irrigation regimen on resin-based sealer penetration and pushout bond strength: Cureus, 2020; 12(4); e7807
27. Camps J, Pashley D, Reliability of the dye penetration studies: J Endod, 2003; 29(9); 592-94
28. Brandao C, De Moraes I, Bramante C, Apical sealing ability of ionomeric endodontic sealers: Rev FOB, 2001; 9(2); 29-34
29. Samson E, Kulkarni S, Sushil KC, Likhitkar M, An in-vitro evaluation and comparison of apical sealing ability of three different Obturation technique – lateral condensation, Obtura II, and Thermafil: J Int Oral Health, 2013; 5(2); 35-43
30. Friedman S, Lost C, Zarrabian M, Evaluation of success and failure after endodontic therapy using a glass ionomer cement sealer: J Endod, 1995; 21(7); 384-90
31. McDougall IG, Patel V, Santerre P, Resistance of experimental glass ionomer cement sealers to bacterial penetration in vitro: J Endod, 1999; 25(11); 739-42
32. Timpawat S, Amornchat C, Trisuwan WR, Bacterial coronal leakage after obturation with three root canal sealers: J Endod, 2001; 27(1); 36-39
33. Pommel L, About I, Pashley D, Apical leakage of four endodontic sealers: J Endod, 2003; 29(3); 208-10
34. Rohde TR, Bramwell JD, Hutter JW, An in vitro evaluation of microleakage of a new root canal sealer: J Endod, 1996; 22(7); 365-68
35. Komabayashi T, Colmenar D, Cvach N, Comprehensive review of current endodontic sealers: Dent Mater J, 2020; 39(5); 703-20
36. Versiani MA, Carvalho-Junior JR, Padilha MI, A comparative study of physicochemical properties of AH Plus and Epiphany root canal sealants: Int Endod J, 2006; 39(6); 464-71
37. Souza SF, Bombana AC, Francci C, Polymerization stress, flow and dentine bond strength of two resin-based root canal sealers: Int Endod J, 2009; 42(10); 867-73
38. Zmener O, Pameijer CH, Serrano SA, Significance of moist root canal dentin with the use of methacrylate-based endodontic sealers: An in vitro coronal dye leakage study: J Endod, 2008; 34(1); 76-79
39. Crozeta BM, Lopes FC, Silva RM, Retreatability of BC Sealer and AH Plus root canal sealers using new supplementary instrumentation protocol during non-surgical endodontic retreatment: Clin Oral Investig, 2021; 25(3); 891-99
40. Patni PM, Chandak M, Jain P, Stereomicroscopic evaluation of sealing ability of four different root canal sealers – an in vitro study: J Clin Diagn Res, 2016; 10(8); 37-39
41. Jeanneau C, Giraud T, Milan JL, About Investigating unset endodontic sealers’ eugenol and hydrocortisone roles in modulating the initial steps of inflammation: Clin Oral Investig, 2020; 24(2); 639-47
42. Teixeira ABV, de Castro DT, Schiavon MA, Dos Reis AC, Cytotoxicity and release ions of endodontic sealers incorporated with a silver and vanadium base nanomaterial: Odontology, 2020; 108(4); 661-68
43. Garg N, Garg A, Kang R, A comparison of apical seal produced by zinc oxide eugenol, metapex, ketac endo and ah plus root canal sealers: Endodontology, 2014; 26; 252-58
Figures
Figure 1. (A) Apical dye leakage after filling with Endomethasone N paste and Thermafil obturator. (B) Apical dye leakage after filling with EndoRez paste and Thermafil obturator. (C) Apical dye leakage after filling with GI sealer and Thermafil obturator.Figure 2. (A) Dye leakage in positive control group. (B) Apical dye leakage in negative control group.Figure 3. Dye leakage level comparation between Endomethasone and GI cement tested groups.Figure 4. Dye leakage level comparation between Endomethasone and EndoRez tested groups.Figure 5. Dye leakage level comparation between glass ionomer cement and EndoRez tested groups. Most Viewed Current Articles
15 Jun 2022 : Clinical Research
Evaluation of Apical Leakage After Root Canal Obturation with Glass Ionomer, Resin, and Zinc Oxide Eugenol ...DOI :10.12659/MSMBR.936675
Med Sci Monit Basic Res 2022; 28:e936675
07 Jul 2022 : Laboratory Research
Cytotoxicity, Apoptosis, Migration Inhibition, and Autophagy-Induced by Crude Ricin from Ricinus communis S...DOI :10.12659/MSMBR.936683
Med Sci Monit Basic Res 2022; 28:e936683
01 Jun 2022 : Laboratory Research
Comparison of Sealing Abilities Among Zinc Oxide Eugenol Root-Canal Filling Cement, Antibacterial Biocerami...DOI :10.12659/MSMBR.936319
Med Sci Monit Basic Res 2022; 28:e936319
08 Dec 2022 : Original article
Use of Estimated Glomerular Filtration Rate and Urine Albumin-to-Creatinine Ratio Based on KDIGO 2012 Guide...DOI :10.12659/MSMBR.938176
Med Sci Monit Basic Res 2022; 28:e938176