16 September 2020: Database Analysis
Outcomes for Patients with Sepsis Following Admission to the Intensive Care Unit Based on Health Insurance Status: A Study from the Medical Information Mart for Intensive Care-III (MIMIC-III) Database
Ying Zhou1ABCDEF*, Di Yang2BCE, Qiang Fu2E, Tao Chen1E, Yong Chen1E, Chuandong Zheng1EGDOI: 10.12659/MSM.924954
Med Sci Monit 2020; 26:e924954






Abstract
BACKGROUND: Previous research has focused on poor outcomes from a lack of insurance, but the effects of different types of insurance for patients with sepsis in the intensive care unit (ICU) have not been well studied. We aimed to investigate whether private health insurance was better than government-run health insurance in the United States in terms of clinical outcomes of patients with sepsis in the ICU.
MATERIAL AND METHODS: Patients with sepsis were identified from the Medical information Mart for Intensive Care-III database. Patients were grouped as having private and government-run health insurance. Clinical outcomes were compared in univariate and multivariate analyses. Propensity score match (PSM) and subgroup analysis were used to check the robustness of results.
RESULTS: Data from 13,957 patients were extracted. After adjustment by multivariate model, the private insurance group had similar rates of ICU mortality (relative risk [RR] [95% confidence interval CI]=1.052 [0.919–1.205], P=.463) and 90-day (RR [95% CI]=.964 [0.885–1.051], P=.406) compared with the group with government-run insurance. The private insurance group had longer ICU stays (strictly standardized mean difference=0.092, P<.001) and better long-term survival (hazard ratio [95% CI]=0.875 [0.825–0.928], P<.001) than the government-run insurance group in the PSM cohorts. Subgroup analysis indicated little variation in results for specific conditions.
CONCLUSIONS: Patients with sepsis who had private insurance had longer ICU stays but similar ICU mortality and 90-day mortality rates than similar patients with government-run insurance; they seemed to have better long-term survival, but more evidence may be required to support this conclusion.
Keywords: database, Hospital Mortality, Insurance, Major Medical, propensity score, Sepsis, Survival Rate, Critical Care, Databases, Factual, Hospitalization, Insurance, Health, Intensive Care Units
Background
Insurance has proven to be associated with the outcomes of patients who have a variety of clinical conditions [1–3]. Previous research has focused on poor outcomes from a lack of insurance [1,4], but the effects of different types of insurance have not been well-studied. Over the years, health insurance coverage has dramatically increased. In 2008, 85.1% of Americans had insurance, versus 91.2% in 2016. In particular, private health insurance coverage was more prevalent than government-run health insurance coverage (67.5% and 37.3%, respectively). For government-run health insurance coverage, the majority of patients had Medicaid (19.4%) and Medicare (16.7%) [5].
Patients with sepsis in the Intensive Care Unit (ICU) are facing life-threatening conditions; the costs are expensive for both patients and the government. Patients with private insurance are more likely to have aggressive therapy that may not be cost-efficient compared to those with government-run insurance [2,6]. For patients in the ICU, that may mean longer mechanical ventilation, longer stays, and more invasive procedures. Not all aggressive strategies are beneficial, in terms of outcomes to every individual. For public health, distribution of medical resources is always an issue. Moreover, because most individuals with government-run insurance have low incomes, are elderly, or have disabilities [7], social equity must be considered. Thus, it is important to determine if government-run health insurance is as good as private health insurance with regard to outcomes of patients in the ICU.
The aim of this study was to explore the effects (both short- and long-term) of different types of health insurance (private and government-run programs) on outcomes of patients with sepsis in the ICU. We hypothesized that individuals with private insurance would have better outcomes than their counterparts in the ICU who had government-run health insurance.
Material and Methods
DATA SOURCE AND CRITERIA:
The Medical Information Mart for Intensive Care-III (MIMIC-III) database was used to identify adult patients with sepsis admitted to the ICU. It is a large, freely available database comprising deidentified health-related data associated with over 40 000 patients admitted to the critical care units of Beth Israel Deaconess Medical Center between 2001 and 2012 [8]. As a result, the informed consent and approval of the Institutional Review Board were waived.
Inclusion and exclusion criteria were: (1) sepsis diagnosis meeting the Angus criteria – simply, patients were suffering from a bacterial or fungal infection plus a diagnosis of acute organ dysfunction [9]; (2) age 18 to 89 years old; (3) first admission to the ICU (if there were multiple admissions for the same patient); and (4) insurance type was not “self-pay”. The dataset size is shown in the analysis flow chart.
FEATURE DATA FOR EXTRACTION:
General information, including admission type (i.e., elective, urgent or emergency, according to the treatment priority); insurance type (i.e., private, government, Medicare and Medicaid); sex; age when admitted to the ICU; first ICU department (i.e., Coronary Care Unit [CCU], Cardiac Surgery Recovery Unit [CSRU], Medical ICU [MICU], Surgical ICU [SICU], or Thoracic Surgery ICU [TSICU]) was extracted from the MIMIC-III database. Medicare and Medicaid were the two main types of government-run insurance. Medicare is a federal program that provides health coverage if an individual is ≥65 years old or <65 years old and has a disability, regardless of income, whereas Medicaid is a state and federal program that provides health coverage if an individual has very low income [7]. Thus, we merged government, Medicare, and Medicaid insurances into government-run insurance for further analyses.
Data on disease severity score systems, including Sequential Organ Failure Assessment (SOFA) [10] and Simplified Acute Physiology Score (SAPS) II [11], were also extracted. For comorbidity evaluation, we extracted the Elixhauser score [12]. Data on vasopressor use and mechanical ventilation information in the first 24 hours after admission to the ICU were also extracted as binomial variables (i.e., yes or no); vasopressors included norepinephrine, epinephrine, phenylephrine, vasopressin, dopamine, dobutamine, and milrinone.
OUTCOMES DATA FOR EXTRACTION:
The primary outcome for the study was ICU mortality. Secondary outcomes were length of ICU stay, 90-day mortality, and long-term survival. The data were acquired from the Social Security Death Index (SSDI). ICU mortality and 90-day mortality served as binomial variables and were considered a “short-term effect.” The two data sources for the MIMIC-III database had different follow-up times (i.e., 90 days for Metavision and 4 years for CareVue) [8,13,14], that is, if no record of death was found in the SSDI, we consider it was censored at the 90th day after admission to ICU for the Metavision data source or at end of the fourth year after admission to the ICU for the CareVue data source. In this way, we used the time-event data to conduct a survival analysis, which was considered as the “long-term effect.”
STATISTICAL METHODS:
Data extracted from the database were first checked for missing data. Since the missing data of all variables were less than 1%, we just deleted the missing data. Baseline data and outcomes grouped by different insurance types – government-run and private – were then summarized for comparison. Continuous data were described by median and quantiles and tested using a nonparametric method (Kruskal-Wallis test), while categorical data were summarized by number and percentages and tested by the chi-square method. Strictly standardized mean differences (SSMDs) were also calculated for all variables. We used multiple methods of analysis to ensure the robustness of our results. First, confounders and lack of balance were adjusted using multivariate analysis and propensity score matching (PSM). The logistic regression model was applied to both methods to calculate the risk ratio for each variable and propensity score for each patient. All variables except outcomes (they were what we predicted) were entered into the model (for propensity score calculation, besides outcomes, insurance type was also not included because it was what we predicted). For PSM, we performed a one-to-one match with calipers less than 0.01 between the two groups and obtained the matched cohorts. The matched cohorts were also compared with univariate and multivariate methods. Second, we performed subgroup analyses for each variable and calculated the risk ratios for both the ICU and 90-day mortality rates. We used forest plots to visualize the subgroup analyses [15]. Finally, the survival analysis was used to compare long-term outcomes between the different types of insurance. Kaplan-Meier curves were plotted and a Cox proportional hazard model was used to adjust for confounders and calculate hazard ratios. For all comparisons, a P<.05 was considered to have statistical significance.
The database was created on the personal computer of the first author with Postgresql 10.1. Data extraction was achieved with Python 3.6 and SQL sentences. The rest of the data analysis process was performed with R language (version 3.6).
Results
We retrieved 13 957 records from the MIMIC-III database that met our extractive criteria. We directly excluded 98 records with incomplete data (less than 1% of the entire dataset). The detailed extraction and analysis process is shown in the flowchart in Figure 1. Baseline data and outcomes for the patients, grouped according to insurance type, are summarized in Table 1. Patients with government-run insurance were elderly more likely to be in the CCU and MICU, more likely to present in the Emergency Department, and had higher SAPS II and Elixhauser scores. Comparatively, private insurance patients were more likely to be male, in the SICU and TSICU, to have longer ICU stays, and to be given mechanical ventilation on the first day of admission to the ICU. Without adjusting for confounders, patients with government-run insurance had higher rates of ICU mortality and 90-day mortality.
Table 1 also shows results of PSM of the cohorts. After matching, the two cohorts were balanced for most variables. Rates of ICU mortality and 90-day mortality were not significantly different. However, patients with private insurance had longer ICU stays (SSMD=.092,
Multivariate analyses of both the original data and matched data are summarized in Table 2. Neither indicated significant differences in rates of ICU mortality and 90-day mortality between the two insurance groups. Subgroup analysis produced similar results: Few subgroups of variables indicated a significant difference between the two insurance groups (Figure 2).
Interestingly, in the long-term survival analysis, median survival time was longer in the private insurance group than in the government-run insurance group, for both the original cohorts (1 005 days
Discussion
We analyzed a public ICU database and explored the effects of different types of insurance types on clinical outcomes of patients with sepsis. We found that patients with private insurance had similar rates of ICU and 90-day mortality but longer stays in the ICU than patients with government-run insurance. Furthermore, long-term survival was better in the private insurance group than in the government-run insurance group.
Previous research has reported on disparities in healthcare services and treatment for a number of clinical conditions in the United States, depending on patient insurance type [2,16,17]. Fouroquet reported lower use of medical services (e.g., hospital, laboratory, pathology and radiology), laparoscopy, and the emergency room for patients with endometriosis who had public health insurance [16]. However, Fouroquet did not compare the prognosis of patients with public health insurance to those with private health insurance. Similarly, Loehrer did not report a disparity in outcomes in patients with colorectal cancer patients based on type of insurance, but he found that patients with government-run insurance had significantly lower rates of resection for colorectal cancer than their counterparts with private insurance [2], which obviously would influence the prognosis. The same trend appeared in infectious disease. Stepanova reported that patients who were positive for Hepatitis C virus were less likely to have private insurance [17], indicating a higher cure rate in that population. In the current study, we found that patients with private insurance had longer ICU stays and were more frequently given mechanical ventilation. All of the above suggest that insurance type influenced clinical decision-making.
Does insurance type affect clinical outcome by changing clinical decision-making? Chakraborty and colleagues analyzed a database of information on patients with acute coronary syndrome and found that the group with private insurance had lower rates of mortality than their counterparts with Medicare and Medicaid [18]. Gabriel et al. analyzed an ICU dataset of patients with nonspecific diagnoses and found that those with private insurance had lower rates of ICU mortality compared to the group with government-run insurance and the noninsured group [19]. Another study of spine trauma found no disparity in mortality rates between insurance types (private
In 2016, private health insurance coverage was more prevalent than government-run health insurance coverage (67.5%
In the current study, we retrospectively analyzed information from the MIMIC-III database and compared private and government-run insurance. Confounding factors and uncertain causal relationships were found, although we used multiple methods of analysis to avoid these issues. In the long-term survival analysis, we found that patients with private insurance had longer survival than those who had government-run insurance, but this long-term effect may be unrelated to their sepsis at time of ICU admission. Furthermore, we were unable to determine whether the type of insurance the patients had might have changed during the rest of their lives.
Conclusions
Analysis of information in the MIMIC-III database indicates that patients with sepsis who had private insurance had longer ICU stays and were more frequently given mechanical ventilation on their first day of admission to the ICU compared with their counterparts with government-run insurance. However, rates of hospital and 90-day mortality were similar in patients with private versus government-run insurance who were critically ill with sepsis, unlike with conditions such as cancer or chronic diseases. Patients with private insurance had better long-term survival compared than did patients with government-run insurance, which might be affected by factors that were hard to evaluate and for which more evidence is required.
Figures
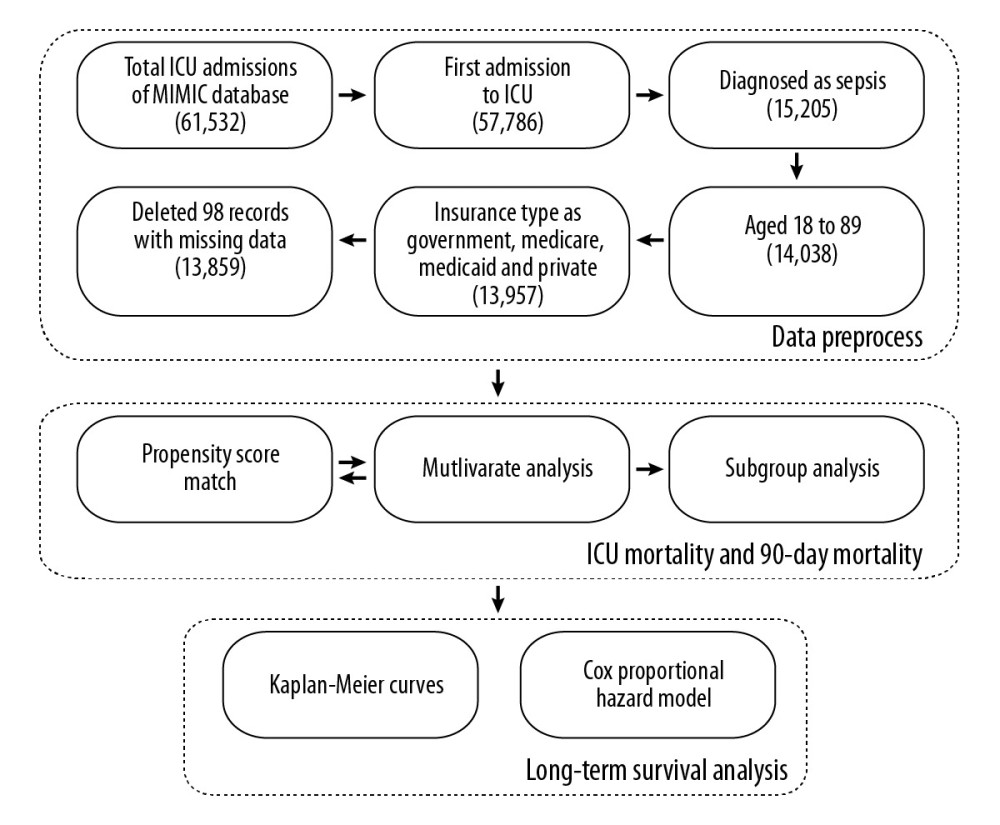 Figure 1. The analysis flow chart of the current study. Data were extracted from the MIMIC-III database. The number of records for each step are in brackets. Multivariate analysis was applied to both unmatched and matched data, so there is a two-way arrow between the propensity score match and multivariate analysis.
Figure 1. The analysis flow chart of the current study. Data were extracted from the MIMIC-III database. The number of records for each step are in brackets. Multivariate analysis was applied to both unmatched and matched data, so there is a two-way arrow between the propensity score match and multivariate analysis. 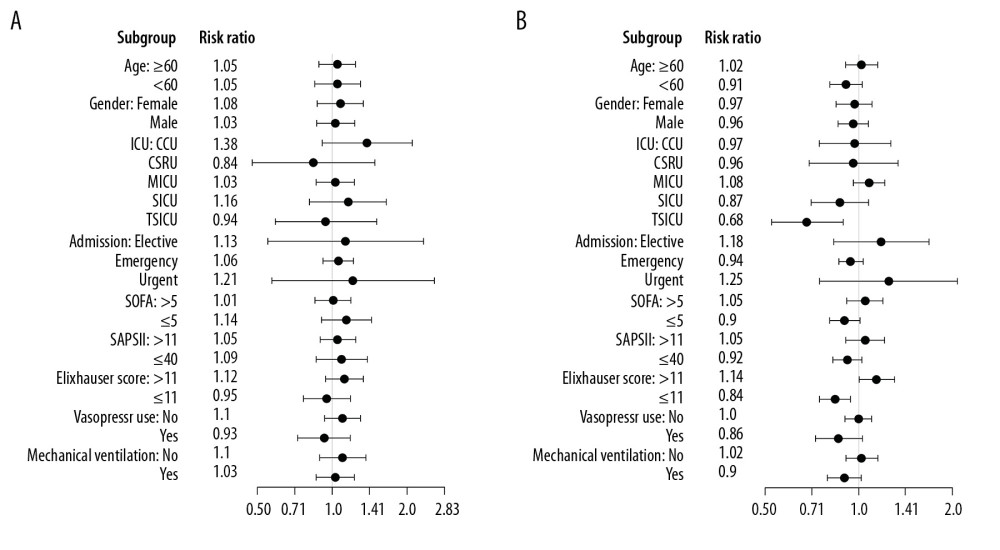 Figure 2. Subgroup analysis of association between insurance type and ICU mortality (A) and 90-day mortality (B) rates. The government-run insurance group is the reference group; risk ratios of the private insurance group are displayed and plotted with their 95% CIs on the right (the forest plot). ICU – Intensive Care Unit; CCU – Cardiac Care Unit; CSRU – Cardiac Surgery Recovery Unit; MICU – Medical ICU; SICU – Surgical ICU; TSICU – Thoracic Surgery ICU; SOFA – Sequential Organ Failure Assessment; and SAPS II – Simplified Acute Physiology Score II.
Figure 2. Subgroup analysis of association between insurance type and ICU mortality (A) and 90-day mortality (B) rates. The government-run insurance group is the reference group; risk ratios of the private insurance group are displayed and plotted with their 95% CIs on the right (the forest plot). ICU – Intensive Care Unit; CCU – Cardiac Care Unit; CSRU – Cardiac Surgery Recovery Unit; MICU – Medical ICU; SICU – Surgical ICU; TSICU – Thoracic Surgery ICU; SOFA – Sequential Organ Failure Assessment; and SAPS II – Simplified Acute Physiology Score II. 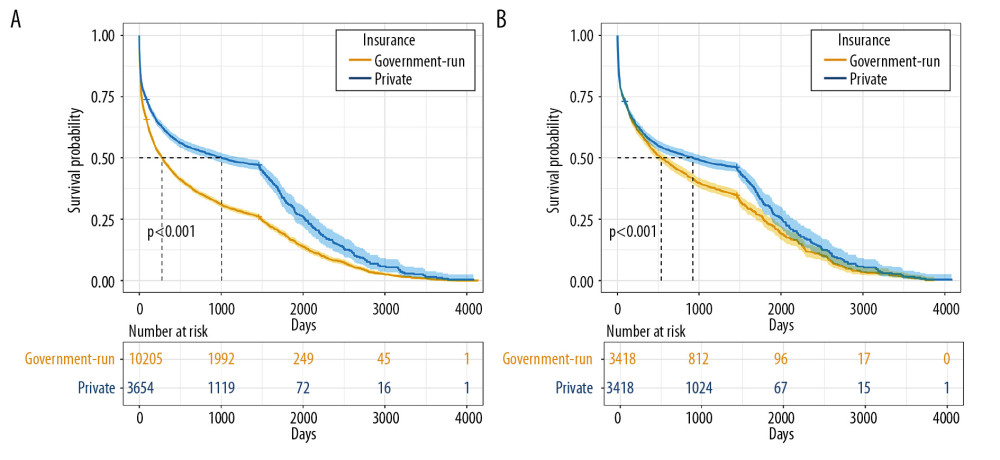 Figure 3. Kaplan-Meier survival curves of patients with different insurance types from the original data (A) and matched data (B). The curves describe the survival probability of each cohort at each day after admission to the ICU to the endpoint (censor or death). Median survival times for the two cohorts from the original data were 277 and 1 005 days, respectively; from the matched data, they were 534 and 924 days, respectively (the horizontal position of the dashed lines). The numbers below the plots refer to the patients at risk of death for every 1 000 days.
Figure 3. Kaplan-Meier survival curves of patients with different insurance types from the original data (A) and matched data (B). The curves describe the survival probability of each cohort at each day after admission to the ICU to the endpoint (censor or death). Median survival times for the two cohorts from the original data were 277 and 1 005 days, respectively; from the matched data, they were 534 and 924 days, respectively (the horizontal position of the dashed lines). The numbers below the plots refer to the patients at risk of death for every 1 000 days. References
1. Kumar G, Taneja A, Majumdar T, The association of lacking insurance with outcomes of severe sepsis: Retrospective analysis of an administrative database: Crit Care Med, 2014; 42(3); 583-91
2. Loehrer AP, Song Z, Haynes AB, Impact of health insurance expansion on the treatment of colorectal cancer: J Clin Oncol, 2016; 34(34); 4110-15
3. Naghavi AO, Echevarria MI, Grass GD, Having Medicaid insurance negatively impacts outcomes in patients with head and neck malignancies: Cancer, 2016; 122(22); 3529-37
4. Lyon SM, Benson NM, Cooke CR, The effect of insurance status on mortality and procedural use in critically ill patients: Am J Respir Crit Care Med, 2011; 184(7); 809-15
5. Bureau USC: Health Insurance Coverage in the United States: 2016, 2018
6. Loehrer AP, Murthy SS, Song Z, Association of insurance expansion with surgical management of thyroid cancer: JAMA Surg, 2017; 152(8); 734-40
7. : Differences between Medicare and Medicaid – Medicare Interactive https://www.medicareinteractive.org/get-answers/medicare-basics/medicare-coverage-overview/differences-between-medicare-and-medicaid
8. Johnson AEW, Pollard TJ, Shen L, MIMIC-III, a freely accessible critical care database: Sci Data, 2016; 3; 160035
9. Angus DC, Linde-Zwirble WT, Lidicker J, Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care: Crit Care Med, 2001; 29(7); 1303-10
10. Vincent JL, Moreno R, Takala J, The SOFA (Sepsis-Related Organ Failure Assessment) score to describe organ dysfunction/failure: Intensive Care Med, 1996; 22(7); 707-10
11. Le Gall JR, Lemeshow S, Saulnier F, A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study: JAMA, 1993; 270(24); 2957-63
12. Quan H, Sundararajan V, Halfon P, Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data: Med Care, 2005; 43(11); 1130-39
13. : Data sources https://mimic.physionet.org/mimicdata/datatypes/
14. : PATIENTS https://mimic.physionet.org/mimictables/patients/
15. Zhang Z, Kossmeier M, Tran US, Rainforest plots for the presentation of patient-subgroup analysis in clinical trials: Ann Transl Med, 2017; 5(24); 485
16. Fourquet J, Zavala DE, Missmer S: Am J Obstet Gynecol, 2019; 221(6); 623.e1-11
17. Stepanova M, Kanwal F, El-Serag HB, Younossi ZM, Insurance status and treatment candidacy of hepatitis C patients: Analysis of population-based data from the United States: Hepatology, 2011; 53(3); 737-45
18. Chakraborty S, Bandyopadhyay D, Amgai B, Does Insurance effect the outcome in patients with acute coronary syndrome?: An insight from the most recent national inpatient sample: Curr Probl Cardiol, 2019 [online ahead of print]
19. Gabriel LEK, Bailey MJ, Bellomo R, Insurance status and mortality in critically ill patients: Crit Care Resusc, 2016; 18(1); 43-49
20. Chan A: Differences between private and public insurance in the United States, 2019
21. Sakr Y, Jaschinski U, Wittebole X, Sepsis in Intensive Care Unit patients: Worldwide data from the intensive care over nations audit: Open Forum Infect Dis, 2018; 5(12); ofy313
Figures
Figure 1. The analysis flow chart of the current study. Data were extracted from the MIMIC-III database. The number of records for each step are in brackets. Multivariate analysis was applied to both unmatched and matched data, so there is a two-way arrow between the propensity score match and multivariate analysis.Figure 2. Subgroup analysis of association between insurance type and ICU mortality (A) and 90-day mortality (B) rates. The government-run insurance group is the reference group; risk ratios of the private insurance group are displayed and plotted with their 95% CIs on the right (the forest plot). ICU – Intensive Care Unit; CCU – Cardiac Care Unit; CSRU – Cardiac Surgery Recovery Unit; MICU – Medical ICU; SICU – Surgical ICU; TSICU – Thoracic Surgery ICU; SOFA – Sequential Organ Failure Assessment; and SAPS II – Simplified Acute Physiology Score II.Figure 3. Kaplan-Meier survival curves of patients with different insurance types from the original data (A) and matched data (B). The curves describe the survival probability of each cohort at each day after admission to the ICU to the endpoint (censor or death). Median survival times for the two cohorts from the original data were 277 and 1 005 days, respectively; from the matched data, they were 534 and 924 days, respectively (the horizontal position of the dashed lines). The numbers below the plots refer to the patients at risk of death for every 1 000 days. Tables
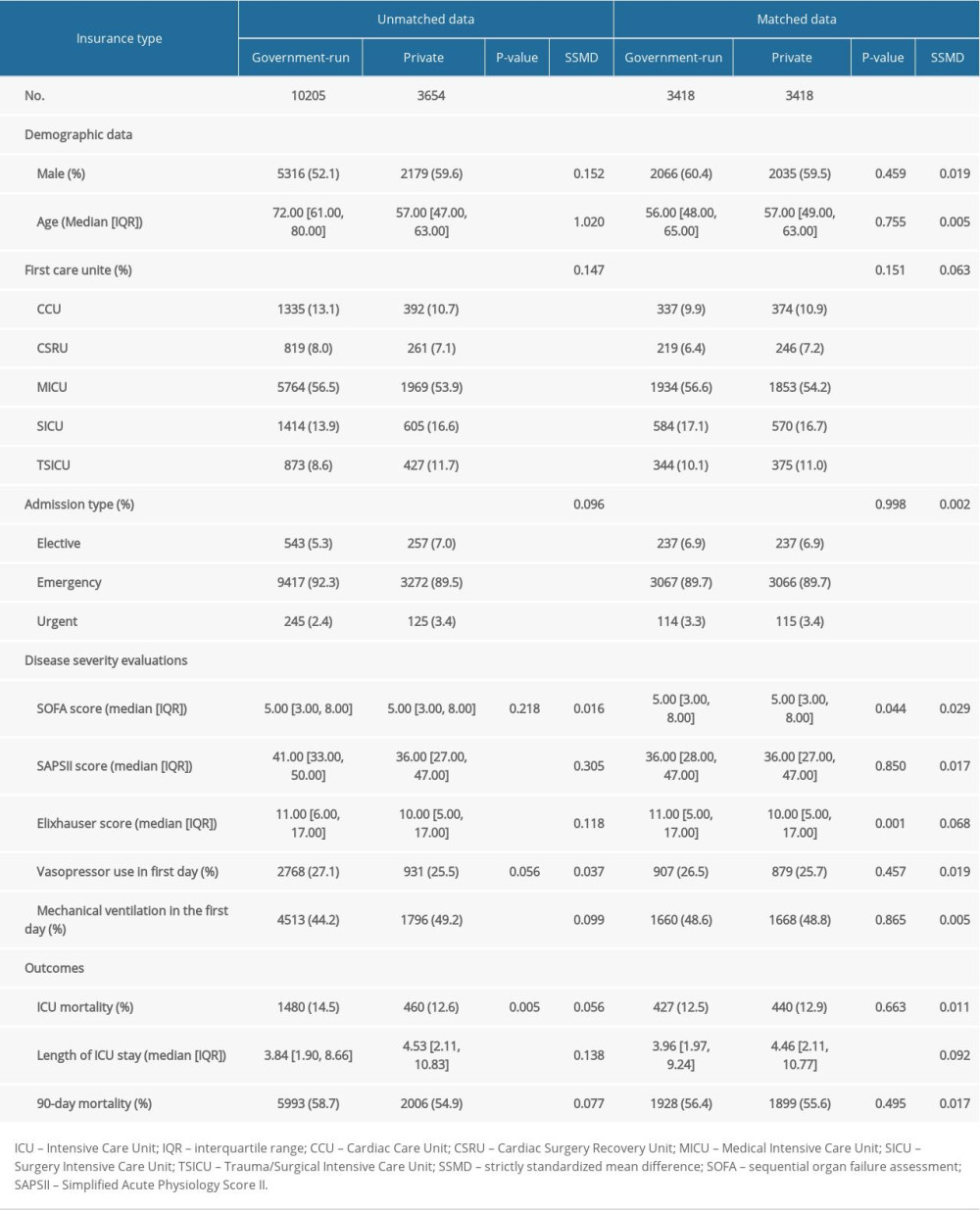 Table 1. Baseline and outcomes of original and propensity-score-matched cohorts with government-run and private insurance.
Table 1. Baseline and outcomes of original and propensity-score-matched cohorts with government-run and private insurance.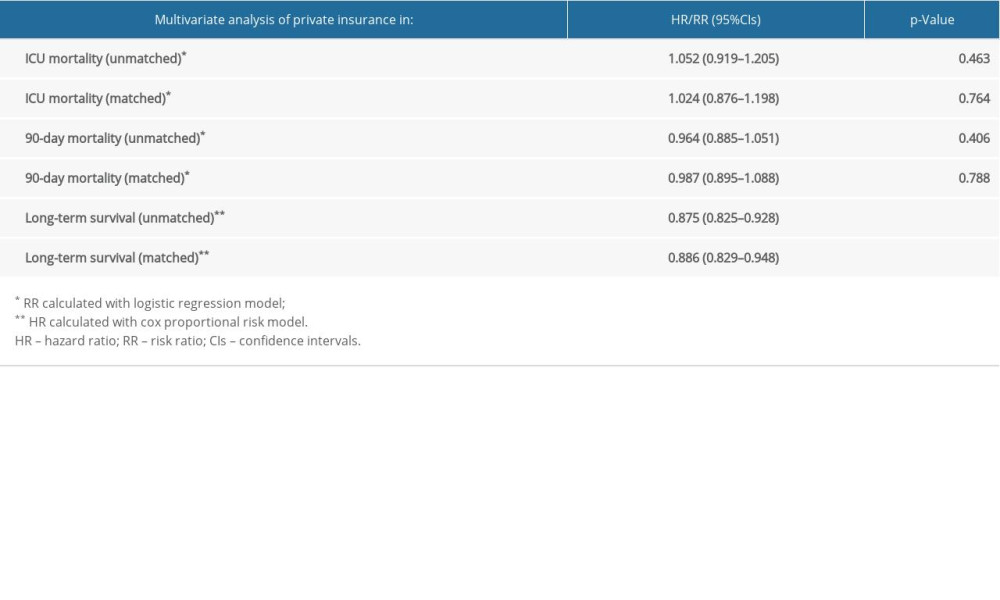 Table 2. Multivariate analysis of private insurance in different cohorts.Table 1. Baseline and outcomes of original and propensity-score-matched cohorts with government-run and private insurance.Table 2. Multivariate analysis of private insurance in different cohorts.
Table 2. Multivariate analysis of private insurance in different cohorts.Table 1. Baseline and outcomes of original and propensity-score-matched cohorts with government-run and private insurance.Table 2. Multivariate analysis of private insurance in different cohorts. In Press
06 Mar 2024 : Clinical Research
Comparison of Outcomes between Single-Level and Double-Level Corpectomy in Thoracolumbar Reconstruction: A ...Med Sci Monit In Press; DOI: 10.12659/MSM.943797
21 Mar 2024 : Meta-Analysis
Economic Evaluation of COVID-19 Screening Tests and Surveillance Strategies in Low-Income, Middle-Income, a...Med Sci Monit In Press; DOI: 10.12659/MSM.943863
10 Apr 2024 : Clinical Research
Predicting Acute Cardiovascular Complications in COVID-19: Insights from a Specialized Cardiac Referral Dep...Med Sci Monit In Press; DOI: 10.12659/MSM.942612
06 Mar 2024 : Clinical Research
Enhanced Surgical Outcomes of Popliteal Cyst Excision: A Retrospective Study Comparing Arthroscopic Debride...Med Sci Monit In Press; DOI: 10.12659/MSM.941102
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952