23 July 2020: Clinical Research
Clinicopathological Analysis and Prognostic Assessment of Transcobalamin I (TCN1) in Patients with Colorectal Tumors
Xinqiang Zhu12ABCDEG*, Kui Yi3BE, Daorong Hou4ADF, Hailong Huang2BC, Xuetong Jiang2ABE, Xiaohong Shi2BCE, Chungen Xing1AEFDOI: 10.12659/MSM.923828
Med Sci Monit 2020; 26:e923828






Abstract
BACKGROUND: Colorectal cancer (CRC) is one of the most common malignancies worldwide. Overall survival (OS) of patients is largely dependent on disease stage at diagnosis and/or surgical resection. TCN1 mainly encodes the vitamin B12 transporter, transcobalamin. Early studies show that TCN1 is a marker of CRC progression, but the impact of TCN1 on survival is unclear.
MATERIAL AND METHODS: We reviewed and analyzed colorectal tumor records, summarized the clinicopathological data, performed immunohistochemical detection of TCN1 again, and semi-quantitatively analyzed protein expression in tumor tissue, non-tumor tissue, and lymph nodes. We followed up patients for 5-year survival.
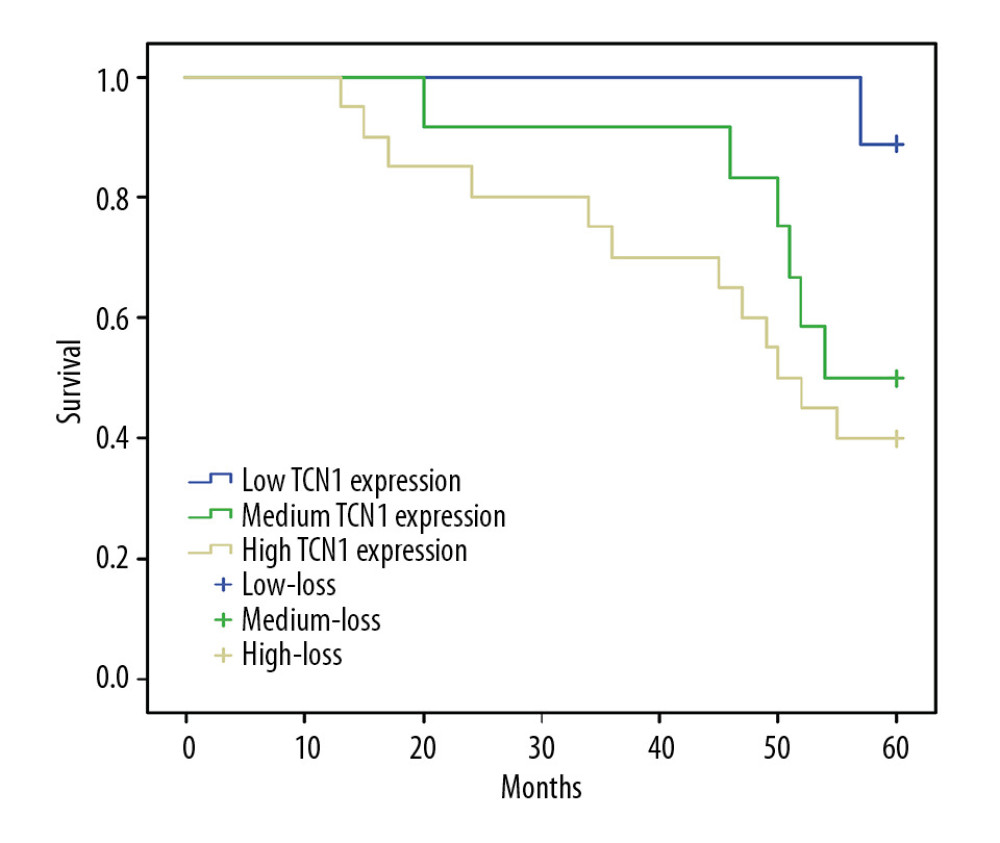
RESULTS: Of 123 patients, 60 (48.7%) had a strong TCN1 immunohistochemical reaction, 36 (29.3%) had a moderate immune response, and 27 (22.0%) had weak expression. The level of immunohistochemical reactivity of TCN1 was correlated with the degree of histological differentiation (H (2.92)=4.976; P=0.083). Survival analysis showed that OS in patients with low TCN1 expression was significantly longer than that in the medium and high TCN1 expression groups (P=0.045). Five-year OS in patients with low, medium, and high TCN1 expression was 88.9%, 50.0%, and 40.0%, respectively. In univariate analysis, TCN1 immune expression was significantly correlated with the 5-year survival rate.
CONCLUSIONS: Although independent risk factors affecting survival of patients with CRC are age, serum CA125, CA19-9, lymph node metastasis, and nerve invasion, negative factors affecting overall 5-year survival in TCN1 should not be ignored, because its high expression suggests a worse clinical prognosis.
Keywords: 14-3-3 Proteins, Colorectal Neoplasms, Pathological Conditions, Anatomical, Aged, 80 and over, Antigens, Tumor-Associated, Carbohydrate, CA-125 Antigen, Follow-Up Studies, Immunohistochemistry, Lymph Nodes, Membrane Proteins, Risk Factors, Survival Rate, Transcobalamins
Background
Colorectal cancer (CRC) is one of the most common malignancies worldwide, and it is the third most common cancer among men and second among women. Multiple factors may contribute to colorectal cancer, including alcohol, smoking, obesity, and lack of exercise [1]. Diagnosis and new treatment options are very advanced, but the clinical outcome in patients with CRC who have locally advanced or metastatic disease remains unsatisfactory. Overall survival (OS) of patients is largely dependent upon disease stage at diagnosis and/or surgical resection [2,3]. Accumulation of various genetic and epigenetic changes in colorectal epithelial cells has also been considered an important factor driving development and progression of CRC [4,5]. It is not difficult to understand why 20% of patients have metastasis at initial diagnosis. Under these circumstances, the 5-year OS rate is less than 15%. Importantly, even the prognosis of patients with primary tumors is unsatisfactory [6,7]. Identifying new methods to describe the high-risk population and applying them clinically has become a huge challenge [8].
Transcobalamin I (TCN1) is a protein with a molecular weight of 60–70 kDa and comes from granulocytic-lineage cells [9,10]. The
Material and Methods
PATIENTS:
A total of 123 patients with colorectal adenocarcinoma admitted to our hospital and Jiangning District People’s Hospital between 2011 and 2014 were retrospectively analysed. Inclusion criteria were (1) colorectal adenocarcinoma, with complete preoperative data and postoperative follow-up data; (2) exposure to adjuvant oxaliplatin/5-fluorouracil/leucovorin were selected; and (3) history of radical surger. Exclusion criteria were: (1) previous history of other malignant tumor; (2) familial adenomatous polyposis; (3) perioperative chemoradiotherapy; (4) intestinal inflammation; and (5) out-of-area metastasis.
From all original medical records, we gathered data on age, sex, tumor location, degree of tumor differentiation, depth of invasion, tumor size, nerve invasion, lymph node metastasis, carcinoembryonic antigen (CEA) level, cancer antigen 125 (CA125) level, and cancer antigen 19-9 (CA19-9) level. The age range of patients was between 39 and 81 years. Tumors were detected in the proximal end of the colon in 30 patients (24.4%), in the distal end in 27 patients (22.0%), and in the rectum in 66 patients (53.6%). Three-grade differentiation was used for grading: 30 cases (24.4%) were well-differentiated (G1), 48 cases (39.0%) were moderately differentiated (G2), and 45 cases (36.6%) were poorly differentiated (G3) (Table 1).
ETHICS AND CONSENT:
We conducted the research according to the Declaration of Helsinki and patients signed informed consent. The study protocol was approved by the Institutional Review Board and Human Ethics Committee of the Affiliated Suqian Hospital of Xuzhou Medical University, Suqian, Jiangsu, China.
IMMUNOHISTOCHEMISTRY PROCEDURES:
Tissues were embedded in paraffin and sectioned, and the sections were deparaffinized and hydrated. Antigen was retrieved with citric acid (pH 6.0), high temperature, and high pressure. Sections were rinsed with phosphate-buffered saline (PBS) and incubated with TCN1 rabbit polyclonal antibody (1: 1000) (Abcam: ab202121) at 4°C overnight. Sections were rinsed with PBS and incubated with secondary antibody (K5004, ready-to-use rapid immunohistochemistry kit, Maixin Biotechnologies, Fuzhou) at room temperature for 20 minutes. Then the sections were rinsed with PBS, developed with 3,3′-diaminobenzidine, counterstained with haematoxylin, and mounted after clearing with xylene.
:
The stained regions and the intensity of the immunohistochemical reaction were primary targets of observation. Quantitative analysis associated with the stained area of the tissue section was as follows: (1) <30% of the cells showed immunoreactivity; (2) 30% to 60% of cells were positive for TCN1; and (3) >60% of the cells were positive. Intensity of the immunohistochemical reaction was quantified as follows: (1) absent or weak; (2) moderate; and (3) strong. The grade of each tissue section was eventually obtained by characterizing the staining area and staining intensity. Expression of TCN1 was given grade 1 for absent/low; grades 2, 3, and 4 for moderate; and grades 6 to 9 for strong reactivity. Evaluation criteria were analyzed by two pathologists using blind methods.
SURVIVAL ANALYSIS:
Survival analysis was performed on the 123 patients, and the survival curve was drawn by the Kaplan-Meier method. Overall survival (OS) was defined as the time from surgery to a patient’s death. Follow-up was for 60 months, although patients who survived beyond 5 years were still followed.
STATISTICAL ANALYSIS:
Statistical analysis was performed using SPSS 17 software. Clinical characteristics of patients’ TCN1 immunoreactivity were assessed with the Kruskal-Wallis test and the Mann-Whitney U test. In addition, Spearman’s rank correlation coefficient was used to assess the relationship between TCN1 immunoexpression and age, CEA level, degree of tumor differentiation, size of primary tumor, and regional lymph node metastasis. The Kaplan-Meier method was used to calculate the survival curve, and the long-rank test technique was used to show the difference in the survival curve.
Results
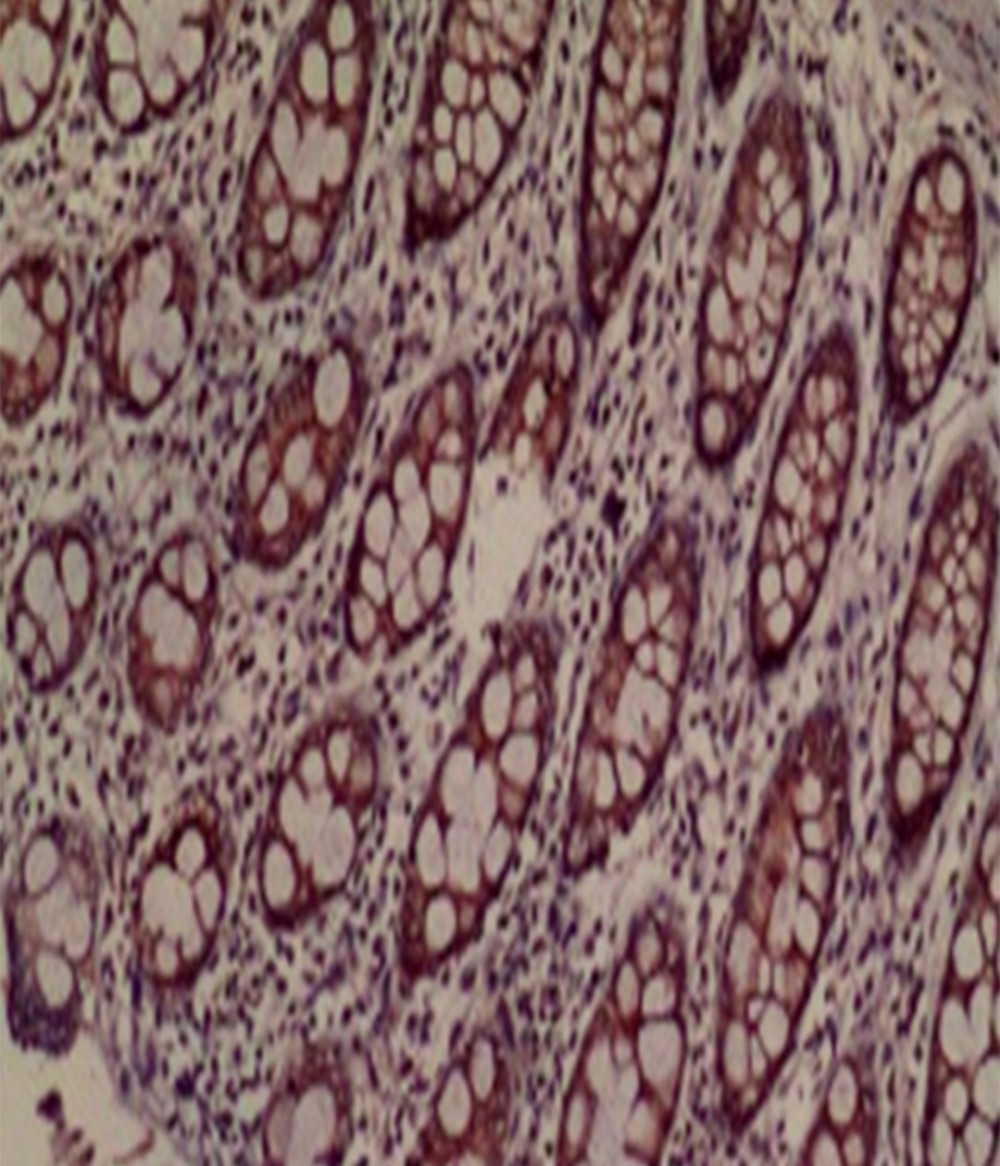
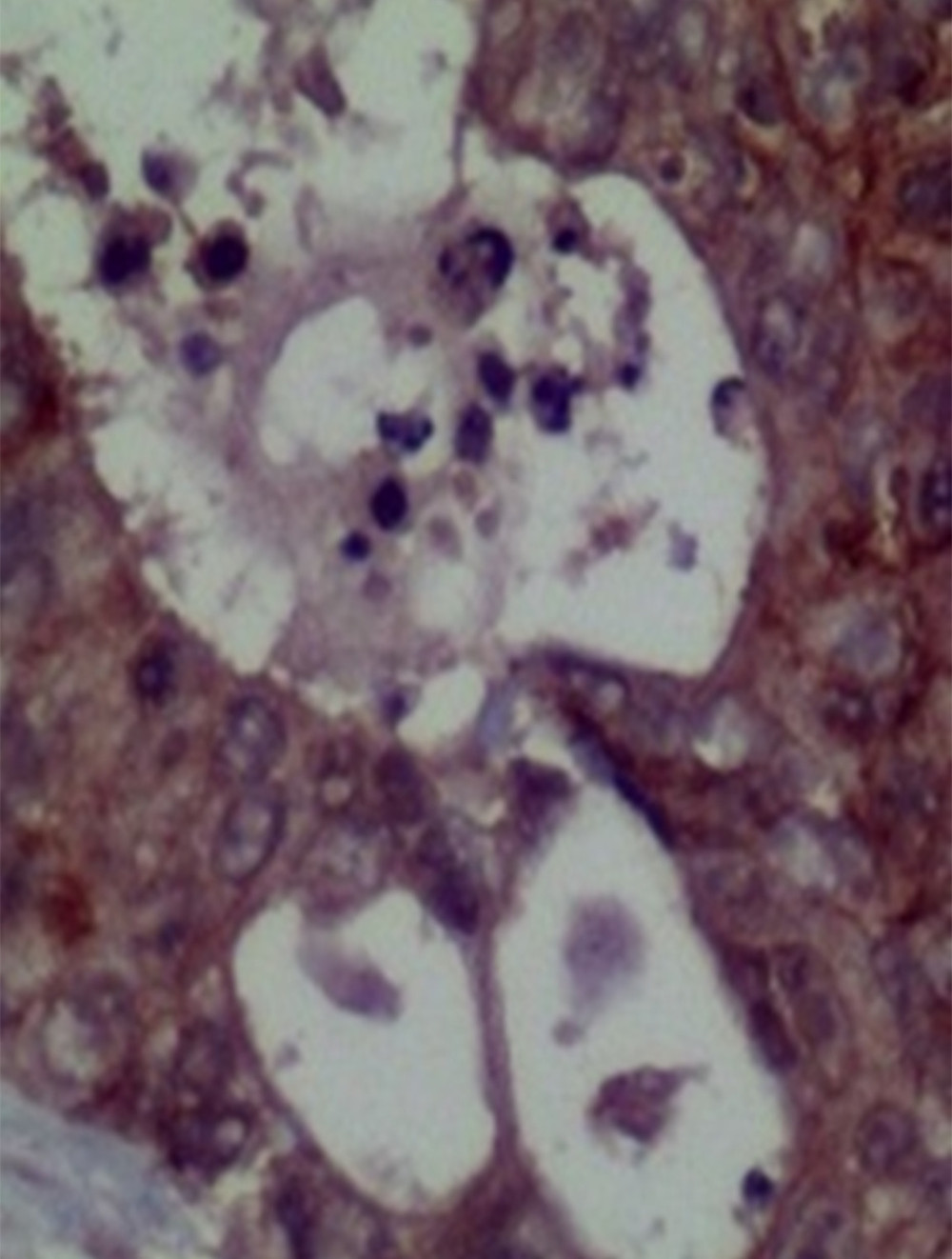
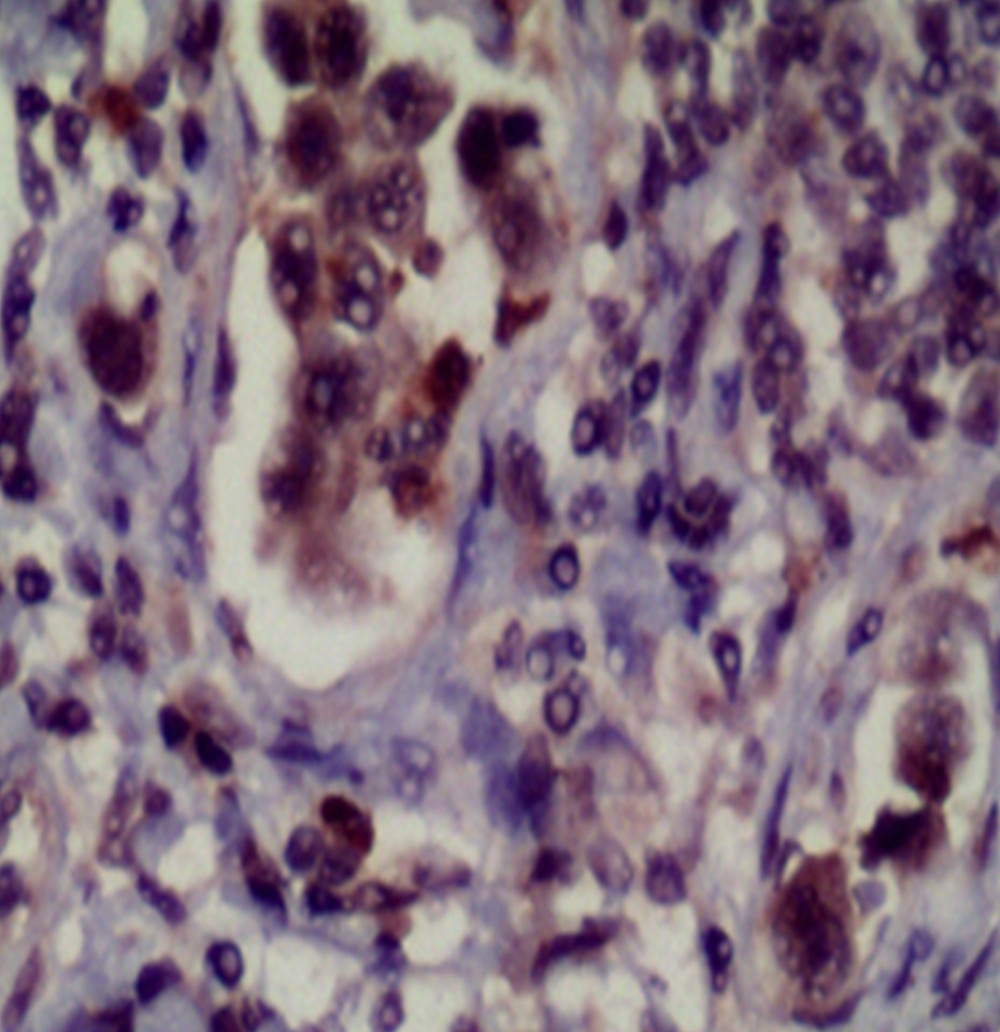
Clinicopathology of TCN1 expression and its relationship with prognosis were analyzed, and CRC tumor tissue was analyzed immunohistochemically. Only trace protein expression was detected in the colorectal mucosa adjacent to non-tumor tissue, whereas high expression was found in poorly differentiated or moderately differentiated tumors and metastatic lymph nodes (Figures 1–3). Of the 123 specimens, 60 (48.7%) had strong TCN1 immunohistochemical reactivity, 36 (29.3%) had moderate reactivity, and 27 (22.0%) had weak TCN1 expression. There was moderate to strong expression of TCN1 in lymph node metastases, and there was also high expression of TCN1 in the para-tumoral nervous tissues.
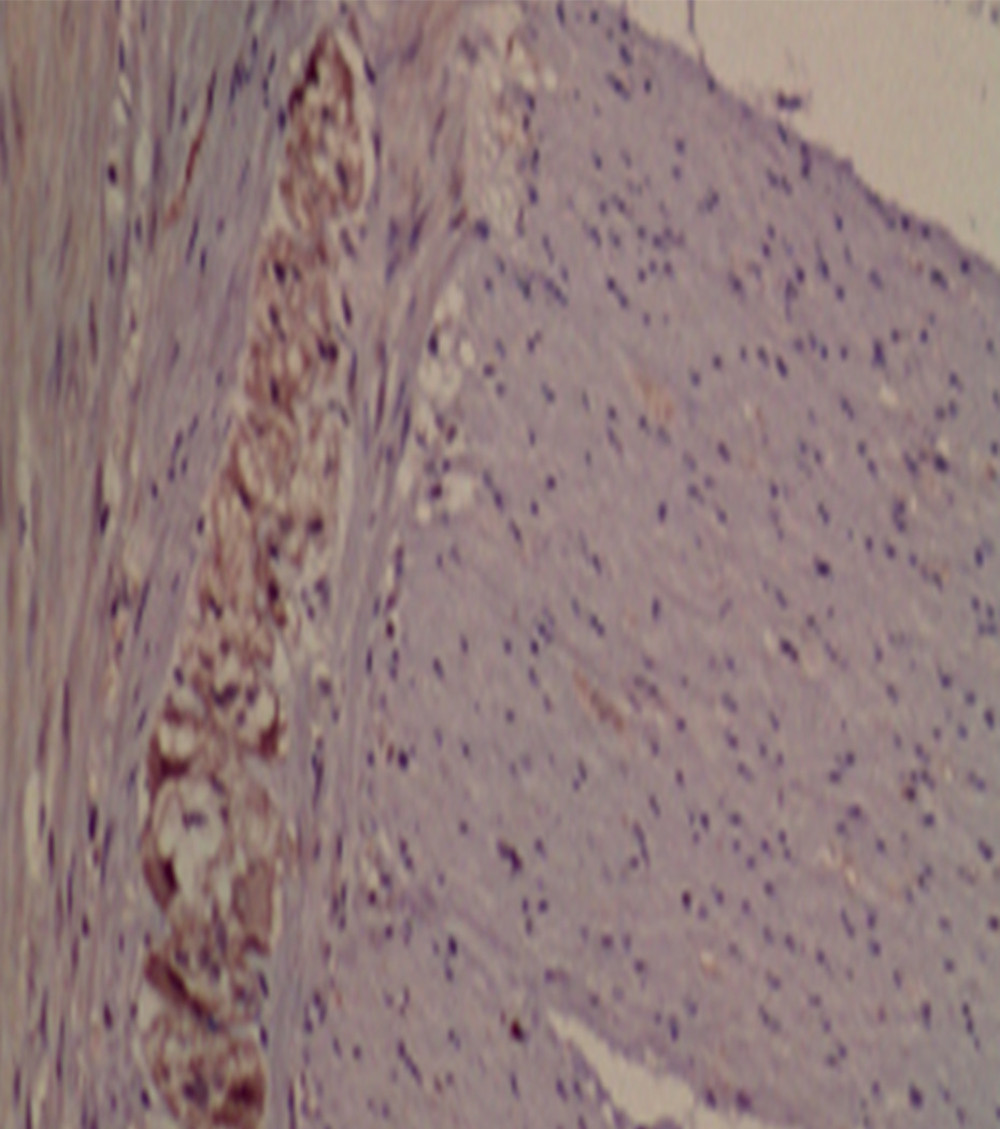
We next calculated whether there was any correlation between TCN1 expression and nerve invasion by tumors (Figure 4). The correlation between the level of TCN1 immunohistochemical reactivity and histological differentiation was
Kaplan-Meier survival analysis showed that OS in patients in the low TCN1 expression group was significantly longer than that in the medium and high TCN1 expression groups (P=0.045; Table 3, Figure 5). Five-year OS rates in patients with low, medium, and high levels of TCN1 immunoexpression were 88.9%, 50.0%, and 40.0%, respectively. The average survival time was 59.667 months (95% confidence interval (CI): 59.051–60.283) in the group with low TCN1 expression, 52.750 months (95% CI: 46.538–58.962) in the group with medium TCN1 expression, and 45.850 months (95% CI: 38.695–53.005) in the group with strong TCN1 expression. The average survival time of all patients was 50.902 months (95% CI: 46.619–55.186; Table 4).
In univariate analysis, CEA, CA125, CA19-9, differentiation degree of tumor, regional lymph node involvement, perineural invasion, size of primary tumor, and TCN1 immunoexpression were significantly associated with lower 5-year survival. However, multivariate analysis showed that only age (HR=4.329; 95% CI: 1.194–15.695; P=0.026), CA125 (HR=3.732; 95% CI: 1.371–10.154; P=0.010), CA19-9 (HR=6.045; 95% CI: 2.017–18.119; P=0.001), regional lymph node metastasis (HR=5.868; 95% CI: 1.546–22.272; P=0.009), and nerve invasion (HR=9.711; 95% CI: 2.403–39.243; P=0.001) were independent risk factors for poor survival. Due to CRC stage in the patients, postoperative adjuvant chemotherapy regimens were different, basically only oxaliplatin/5-FU. Only a small number of patients with early-stage disease did not receive chemotherapy, and the difference was not statistically significant compared with those receiving chemotherapy (Table 5).
Discussion
CORRELATION BETWEEN TCN1 AND CLINICOPATHOLOGY OF COLORECTAL TUMOURS:
In this study, we found that TCN1 protein was highly expressed in both primary colorectal adenocarcinomas and lymph node metastases. In addition, high levels of TCN1 immunoexpression in tumor tissues are strongly associated with clinicopathological factors related to malignant tumors and 5-year OS. High expression of TCN1 is significantly correlated with tumor grading in advanced disease. Statistical results of Kruskal Wallis showed that there was a statistically significant difference between G1 stage tumors and G2 stage tumors, and between G1 stage tumors and G3 stage tumors. In both groups, patients with stage 3 tumors were characterized by high levels of TCN1 expression (R=0.353; P=0.024). The Mann-Whitney U test and Spearman’s rank correlation coefficient showed that strong TCN1 expression was correlated with increased CEA, tumor enlargement, greater degree of invasion, and presence of lymph node metastasis, suggesting that this protein may be involved in the development and progression of malignant tumors. For example, upregulation of TCN1 in the cytoplasm of tumor tissues has been reported, and TCN1 is overexpressed in several malignant tumors, such as hepatocellular carcinoma and breast, lung, and gastric cancers [14,15]. In semi-quantitative analysis, TCN1 was also highly expressed in nervous system tissue, which also showed that TCN1 could be a good indicator of nerve invasion and provide good evidence for metastasis of tumour to the nervous system. Recently, a bioinformatics-based study showed that TCN1 is an important oncogene for normal and CRC tissue classification [16]. The high expression of TCN1 in lymph node metastases may indicate that colorectal cancer cells expressing TCN1 have greater metastatic ability. Increased TCN1 immunoexpression has been associated with decreased OS in patients with CRC. In gastric cancer studies, TCN1 was significantly correlated with gastric cancer stage, cell differentiation, lymph node metastasis, and prognosis [18]. The effect of TCN1 on survival of patients with different tumors also varies. Increased expression in gastrointestinal tumors suggests poor survival, while in liver tumors, the correlation was the opposite [19], suggesting that the mechanism of TCN1 in different solid tumors may not be identical. However, multivariate analysis showed that TCN1 was not an independent risk factor for CRC prognosis. TCN1 is a poorly studied protein but has not been reported to be associated with colorectal cancer. Further studies will help us to better understand its role in colorectal cancer and discover its different pathways of action, not to mention that it may influence tumors through more than one pathway.
ANALYSIS OF FACTORS AFFECTING THE SURVIVAL OF PATIENTS WITH COLORECTAL CANCER:
Colorectal cancer develops fast. It afflicts patients of all ages. The patients in our study included many both young and elderly. Epidemiologic studies have shown that the median age of patients at diagnosis of CRC is 69 years, 90% of those who are diagnosed are older than 50 years, and incidence increases with age. The incidence increases significantly in people over 65, and it can be as high as 176/100 000 people [20]. In this study, patients under 65 accounted for a relatively large proportion, 63.4%, which was related to the small sample size. In different age groups, the pathological nature of the tumor is also different. Poorly differentiated adenocarcinoma accounts for only 10% of cases in elderly patients. Although this proportion is small, poorly differentiated adenocarcinoma has a high degree of malignancy. Coupled with related factors such as age, the prognosis is expected to be relatively poor, making this a problem worthy of our attention [21]. Moreover, the general health status of the elderly is relatively poor, so for most patients, the tumor can go unnoticed and already reach an advanced stage at the time of examination, and tumor invasion is more obvious, which reduces patient survival.
Levels of hematological markers, such as CEA, CA125, and CA19-9, are reliably higher in CRC patients, and their elevated values often indicate a high degree of tumor malignancy, poor differentiation, and susceptibility to metastasis [22]. In advanced CRC, high perioperative expression often indicates distant metastasis [23,24]. However, CEA is not very specific, not sensitive for early diagnosis, and can only be used as an auxiliary means of diagnosing primary malignant tumors with metastasis and postoperative recurrence of tumors. Therefore, in the analysis of this group of patients, it cannot be used as an independent risk factor that affects survival. Nakata et al. [25,26] found that serum CA125 levels were higher in patients with gastrointestinal tumours that had metastasized, suggesting a strong correlation between the two. High expression of CA19-9 in tumors that are rapidly progressing and metastasize to distant locations can be used to predict tumor stage, and the higher the detected value, the greater the accuracy. Multivariate regression analysis in our patients revealed that both CA125 and CA19-9 were correlated with patient survival. Higher initial levels of both parameters suggest a poor clinical prognosis, which is different from the clinical significance reflected by CEA.
Cancer cells can metastasize and spread to lymph nodes through microlymphatic vessels, which is an important step in tumor cell invasion and metastasis. In tumor tissue, the newly formed lymphatic vessel cells form a monolayer, which has a loose connection and no intact basement membrane. In this case, with tumor hyperplasia, the interstitial pressure of the tissue increases and extrudes the lymphatic vessels that have not yet completely formed, so the intercellular space around the monolayer endothelial cells is increased, and its resistance to tumor cells is decreased, which provides a favorable channel for metastasis of tumor cells [27]. Regional lymph node metastasis leads to disease progression in patients and affects their survival.
Nerve invasion was also a risk factor for patient survival in this study. The enteric neural network guides tumor cell migration, in part through the L1 cell adhesion molecule (L1CAM) and N-cadherin [28]. These results open new avenues to study the underlying mechanisms and progression of nerve invasion by CRC. In our TCN1 immunohistochemistry study, we also found that there was higher expression of TCN1 in nervous system tissue. TCN1 has a functional relationship with vitamin B12, and vitamin B12 plays an important role in maintaining nervous system function, hematopoiesis, and cellular metabolism [14,29,30]. There was no statistical significance in the relationship between TCN1 and nerve invasion in this group, which may be related to our low number of clinical medical records.
Conclusions
In summary, high expression of TCN1 in colorectal tumor tissue has many correlations with clinicopathological factors in patients. Although independent risk factors affecting patient survival are age, serum CA125, CA19-9, lymph node metastasis, and nerve invasion, the negative effect of TCN1 on 5-year OS cannot be ignored, and high expression of TCN1 indicates a worse clinical prognosis.
Tables
Table 1. Clinicopathologic data.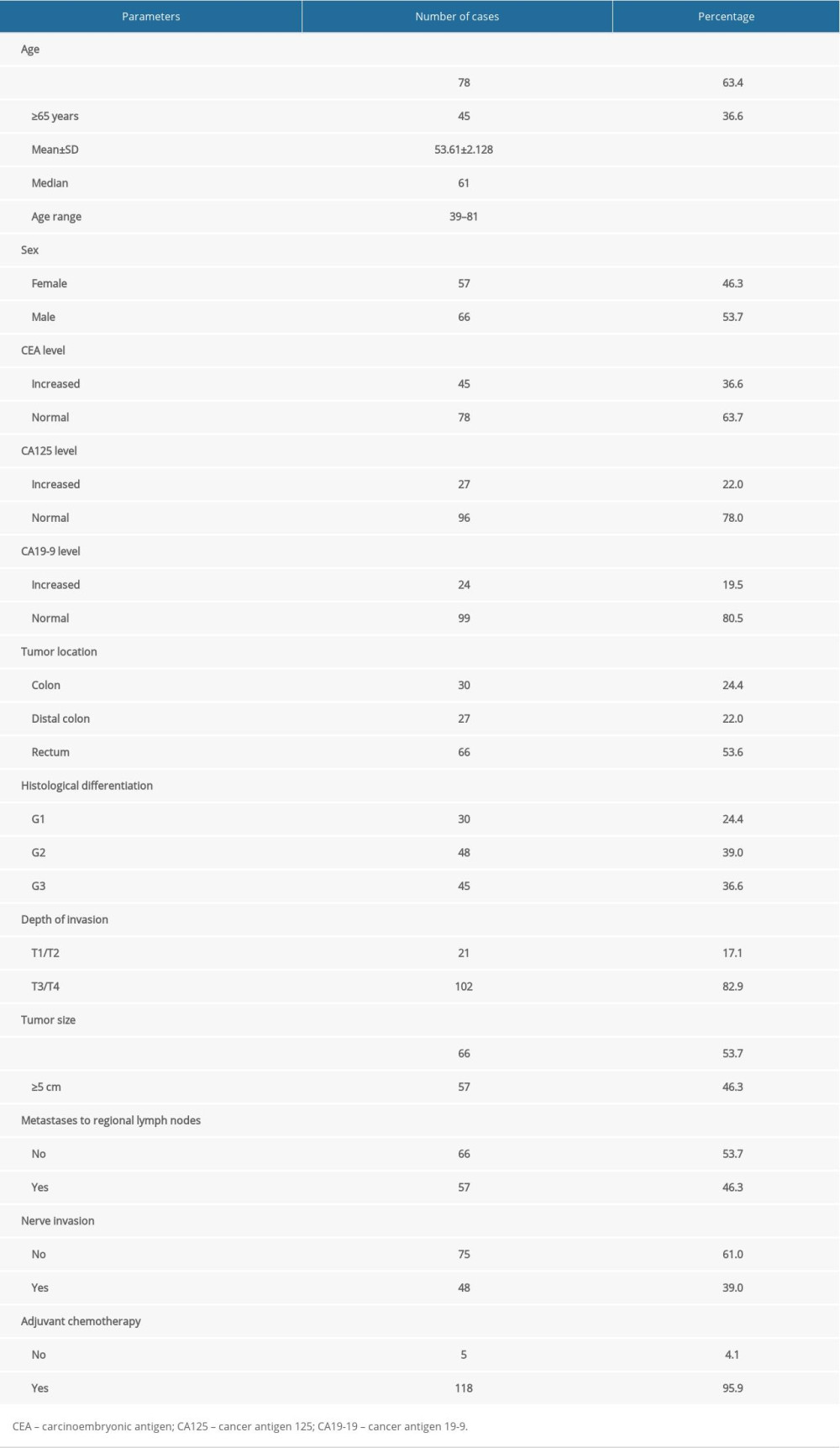 Table 2. Relationship between TCN1 immunoexpression and clinicopathological characteristics in patients with colorectal cancer.
Table 2. Relationship between TCN1 immunoexpression and clinicopathological characteristics in patients with colorectal cancer.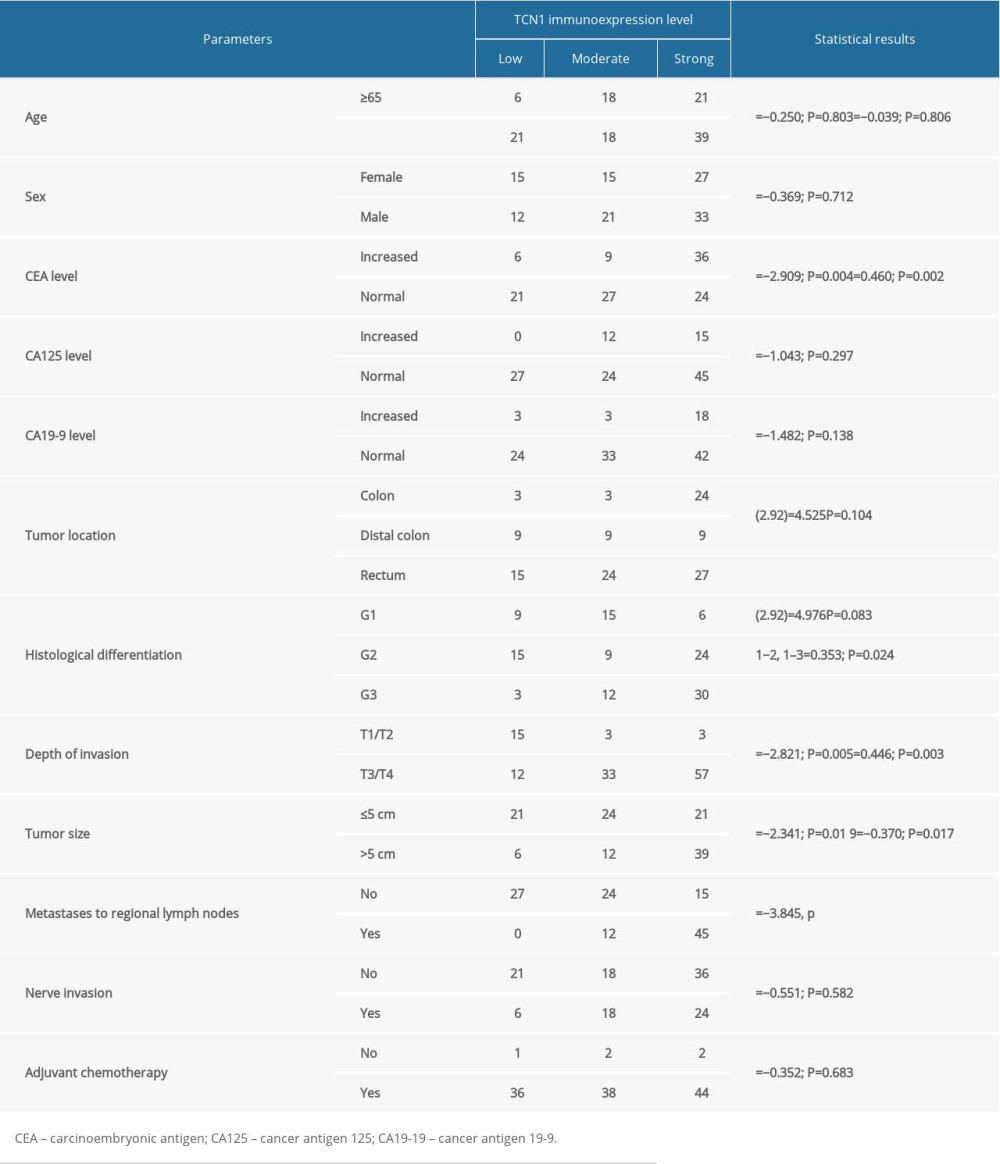 Table 3. Results of survival analysis.
Table 3. Results of survival analysis.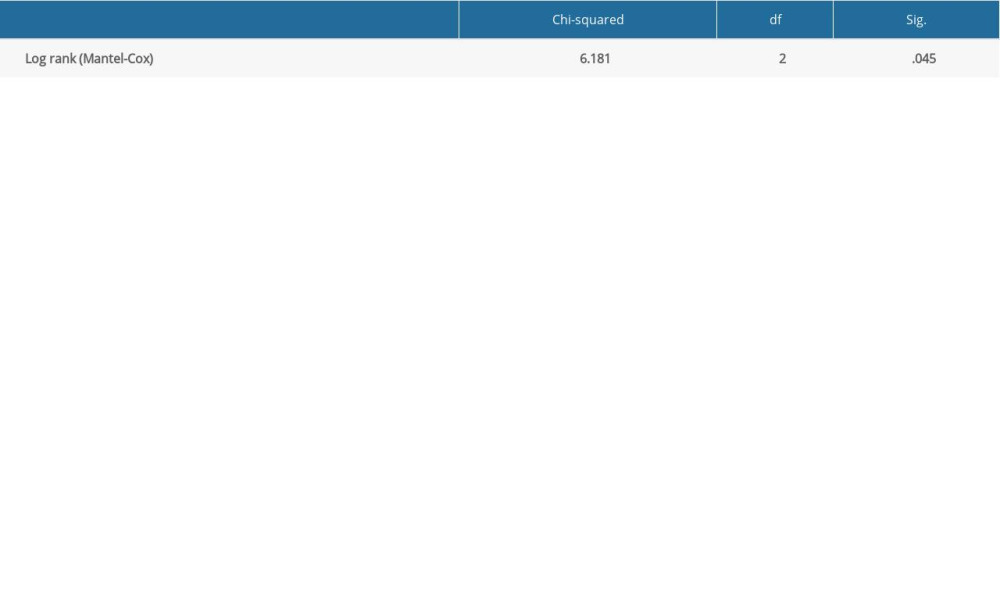 Table 4. Survival time in patients with different TCN1 expression levels.
Table 4. Survival time in patients with different TCN1 expression levels.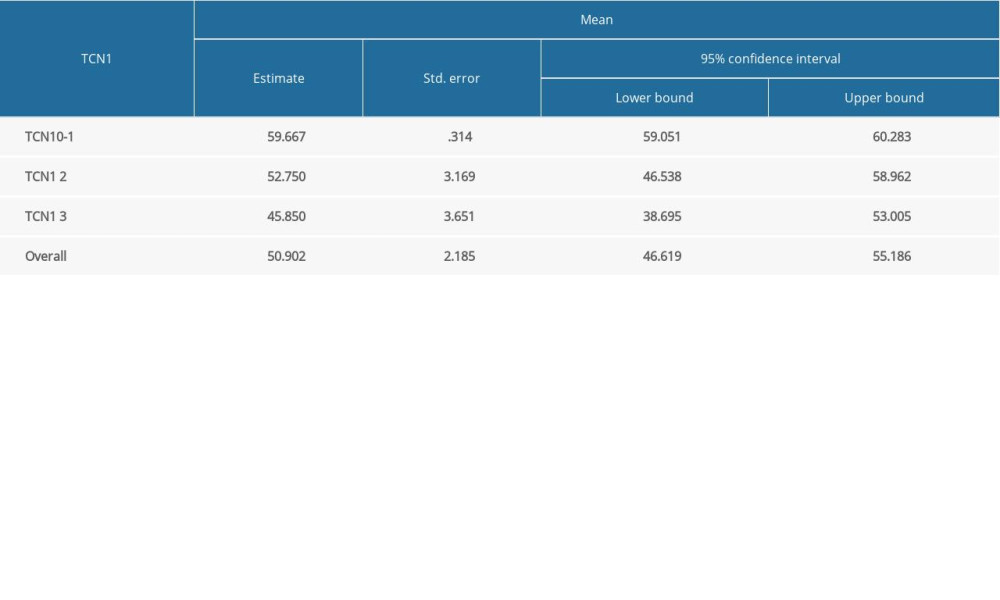 Table 5. Multivariate analysis of various prognostic parameters in CRC patients with Cox regression analysis.
Table 5. Multivariate analysis of various prognostic parameters in CRC patients with Cox regression analysis.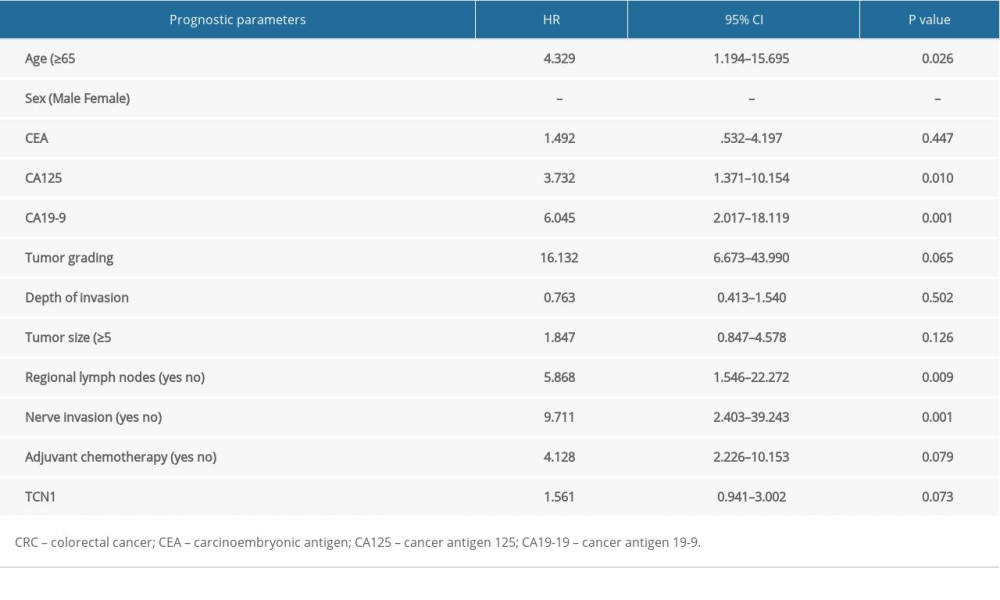
References
1. Fearon ER, Molecular genetics of colorectal cancer: Annu Rev Pathol, 2011; 6; 479-507
2. Muller MF, Ibrahim AE, Arends MJ, Molecular pathological classification of colorectal cancer: Virchows Arch, 2016; 469(2); 125-34
3. Ahmed S, Johnson K, Ahmed O, Advances in the management of colorectal cancer: From biology to treatment: Int J Colorectal Dis, 2014; 29(9); 1031-42
4. Iurlaro R, Leon-Annicchiarico CL, Munoz-Pinedo C, Regulation of cancer metabolism by oncogenes and tumour suppressors: Methods Enzymol, 2014; 542; 59-80
5. Liu J, Li H, Sun L, Aberrantly methylated-differentially expressed genes and pathways in colorectal cancer: Cancer Cell Int, 2017; 17; 75
6. Mody K, Bekaii-Saab T, Clinical trials and progress in metastatic colon cancer: Surg Oncol Clin N Am, 2018; 27(2); 349-65
7. Alwers E, Jia M, Kloor M, Associations between molecular classifications of colorectal cancer and patient survival: A systematic review: Clin Gastroenterol Hepatol, 2019; 17(3); 402-410.e2
8. Minoo P, Zlobec I, Peterson M, Characterization of rectal, proximal and distal colon cancers based on clinicopathological, molecular and protein profiles: Int J Oncol, 2010; 37(3); 707-18
9. Andres E, Serraj K, Zhu J, The pathophysiology of elevated vitamin B12 in clinical practice: QJM, 2013; 106(6); 505-15
10. Gimsing P, Overballe-Petersen C, Hippe E, Cobalamin and cobalamin-binding proteins in plasma related to the clinical condition in chronic myelogenous leukaemia: Leukaemia, 1995; 9(9); 1604-9
11. Shows TB, Alders M, Bennett S, Report of the Fifth International Workshop on Human Chromosome 11 Mapping 1996: Cytogenet Cell Genet, 1996; 74(1–2); 1-56
12. Johnston J, Bollekens J, Allen RH, Structure of the cDNA encoding transcobalamin I, a neutrophil granule protein: J Biol Chem, 1989; 264(27); 15754-57
13. Johnston J, Yang-Feng T, Berliner N, Genomic structure and mapping of the chromosomal gene for transcobalamin I (TCN1): Comparison to human intrinsic factor: Genomics, 1992; 12(3); 459-64
14. Chong LY, Cheok PY, Tan WJ, Keratin 15, transcobalamin I and homeobox gene Hox-B13 expression in breast phyllodes tumours: Novel markers in biological classification: Breast Cancer Res Treat, 2012; 132(1); 143-51
15. Waibel R, Treichler H, Schaefer NG, New derivatives of vitamin B12 show preferential targeting of tumours: Cancer Res, 2008; 68(8); 2904-11
16. Chu CM, Yao CT, Chang YT, Gene expression profiling of colorectal tumours and normal mucosa by microarrays meta-analysis using prediction analysis of microarray, artificial neural network, classification, and regression trees: Dis Markers, 2014; 2014 634123
17. Brzozowa-Zasada M, Kurek J, Piecuch A, The clinical and prognostic evaluation of GRP94 immunoexpression in Caucasian patients with colorectal adenocarcinoma: Prz Gastroenterol, 2019; 14(2); 140-47
18. Kim B, Koo H, Yang S, TC1(C8orf4) correlates with Wnt/beta-catenin target genes and aggressive biological behaviour in gastric cancer: Clin Cancer Res, 2006; 12(11 Pt 1); 3541-48
19. Nagy A, Lanczky A, Menyhart O, Validation of miRNA prognostic power in hepatocellular carcinoma using expression data of independent datasets: Sci Rep, 2018; 8(1); 9227
20. Day LW, Velayos F, Colorectal cancer of the elderly: Curr Treat Options Gastroenterol, 2014; 12(3); 269-82
21. Tao K, Gao J, Wang GClinicopathological characteristics of colorectal carcinoma in the elderly: Zhonghua Wei Chang Wai Ke Za Zhi, 2016; 19(5); 495-98 [in Chinese]
22. Wu XZ, Ma F, Wang XL, Serological diagnostic factors for liver metastasis in patients with colorectal cancer: World J Gastroenterol, 2010; 16(32); 4084-88
23. Yu H, Son GM, Joh YG, The clinical significance of preoperative serum levels of carbohydrate antigen 19-9 in colorectal cancer: J Korean Surg Soc, 2013; 84(4); 231-37
24. Liu F, Yu J, Liang YZAssociated risk factors of peritoneal metastasis in colorectal cancer: Zhonghua Wei Chang Wai Ke Za Zhi, 2011; 14(4); 254-56 [in Chinese]
25. Nakata B, Hirakawa YSCK, Kato Y, Serum CA 125 level as a predictor of peritoneal dissemination in patients with gastric carcinoma: Cancer, 1998; 83(12); 2488-92
26. Sakamoto K, Haga Y, Yoshimura R, Comparative effectiveness of the tumour diagnostics, CA 19-9, CA 125 and carcinoembryonic antigen in patients with diseases of the digestive system: Gut, 1987; 28(3); 323-29
27. Mu J, Yan X, Li ZCharacteristics and clinicopathologic significance of lymphangiogenesis in colorectal cancer: Zhonghua Bing Li Xue Za Zhi, 2005; 34(6); 348-52 [in Chinese]
28. Duchalais E, Guilluy C, Nedellec S, Colorectal cancer cells adhere to and migrate along the neurons of the enteric nervous system: Cell Mol Gastroenterol Hepatol, 2018; 5(1); 31-49
29. Lee YY, Wei YC, Tian YF, Overexpression of Transcobalamin 1 is an independent negative prognosticator in rectal cancers receiving concurrent chemoradiotherapy: J Cancer, 2017; 8(8); 1330-37
30. Morkbak AL, Poulsen SS, Nexo E, Haptocorrin in humans: Clin Chem Lab Med, 2007; 45(12); 175-59
Figures
Tables
Table 1. Clinicopathologic data.Table 2. Relationship between TCN1 immunoexpression and clinicopathological characteristics in patients with colorectal cancer.Table 3. Results of survival analysis.Table 4. Survival time in patients with different TCN1 expression levels.Table 5. Multivariate analysis of various prognostic parameters in CRC patients with Cox regression analysis.Table 1. Clinicopathologic data.Table 2. Relationship between TCN1 immunoexpression and clinicopathological characteristics in patients with colorectal cancer.Table 3. Results of survival analysis.Table 4. Survival time in patients with different TCN1 expression levels.Table 5. Multivariate analysis of various prognostic parameters in CRC patients with Cox regression analysis. In Press
06 Mar 2024 : Clinical Research
Comparison of Outcomes between Single-Level and Double-Level Corpectomy in Thoracolumbar Reconstruction: A ...Med Sci Monit In Press; DOI: 10.12659/MSM.943797
21 Mar 2024 : Meta-Analysis
Economic Evaluation of COVID-19 Screening Tests and Surveillance Strategies in Low-Income, Middle-Income, a...Med Sci Monit In Press; DOI: 10.12659/MSM.943863
10 Apr 2024 : Clinical Research
Predicting Acute Cardiovascular Complications in COVID-19: Insights from a Specialized Cardiac Referral Dep...Med Sci Monit In Press; DOI: 10.12659/MSM.942612
06 Mar 2024 : Clinical Research
Enhanced Surgical Outcomes of Popliteal Cyst Excision: A Retrospective Study Comparing Arthroscopic Debride...Med Sci Monit In Press; DOI: 10.12659/MSM.941102
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952