21 April 2022: Human Study
Case-Control Study to Evaluate the Oral Hygiene Habits in 31 Children with Hemophilia in Bulgaria Using the Oral Health Impact Profile-14 (OHIP-14) Questionnaire
Viktoriya D. Mandova1BCDFG*, Rumen S. Stefanov1ACEDOI: 10.12659/MSMBR.936560
Med Sci Monit Basic Res 2022; 28:e936560






Abstract
BACKGROUND: For patients with hereditary coagulopathies such as hemophilia, the most common dental problem is spontaneous oral bleeding caused by daily oral hygiene habits like tooth brushing. Because of fear of bleeding, children with hemophilia often skip routine oral hygiene procedures, which can lead to dental caries and periodontal diseases. This case control study aimed to evaluate the oral hygiene awareness and hygiene practices of children with hemophilia from 6 to 18 years of age in Bulgaria.
MATERIAL AND METHODS: This study was conducted over 4 years and included 31 patients (children). A sociological approach was used, with direct individual questionnaires for self-assessment of dental habits. Statistical analyses were performed using SPSS.
RESULTS: There was no significant difference between groups in methods of oral hygiene. The duration of oral hygiene procedures was 1 min (n=5, 16.13±6.61%) or 2 min (n=13, 41.94±8.86%), which was considered insufficient for proper oral hygiene. Children who had received oral hygiene advice by a dentist brushed their teeth significantly longer (n=9, 69.23±12.80%) than those who had not. There was a considerable difference between the reasons for the last dental visit between the groups of children (χ²=5.18, P<0.05).
CONCLUSIONS: Children with hemophilia have high awareness of oral hygiene methods; however, more attention should be focused on additional individual educational methods at the dental office. Frequent professional and self-assessment of the oral hygiene routine of children with hemophilia could identify the factors compromising dental status in this vulnerable population.
Keywords: Dental D, Hygiene, Dental Care for Children, Bulgaria, Case-Control Studies, Child, Dental Caries, Habits, Hemophilia A, Humans, Oral Health, Oral Hygiene, Surveys and Questionnaires
Background
Oral health deterioration is a significant problem. Oral health also has an effect on chronic diseases, such as hereditary coagulopathies. The compartmentalization of viewing dental diseases as separate from the general diseases must stop because oral health affects general health by causing considerable pain and suffering. Impaired dental health causes changes in people’s daily diet, speech, quality of life, and well-being [1–3].
At present, few studies have evaluated the relationship between the dental status of people with hemophilia and their chronic disease [4–10]. Limited social activity and compromised oral health has been shown to exist in cases of comorbidity [5,9]. For these patients, the most common dental problem is spontaneous oral bleeding caused by daily oral hygiene habits, such as tooth brushing [4,5]. Fear of inducing bleeding in the oral cavity is the reason many people underestimate their oral hygiene care [4,5]. Once a dental disease is present, dental care for patients with hemophilia can become more complicated and expensive. Chronic diseases discovered in early childhood, including hemophilia, have been reported as an additional risk factor for the development of dental diseases in children [7]. Controversy exists about whether there is better oral health in the deciduous dentition of children with hemophilia or in control groups because patients with hemophilia tend to be from families with lower social status, which is a well-known determinant of higher cariogenicity, especially in young children [8,10]. However, differences in oral status decrease and even become insignificant when comparing groups of adults [11]. Because dental caries and periodontitis are diseases in which health determinants accumulate over time, such as various bacteria and poor oral hygiene techniques, in order to clarify the differences in oral status in children and adults, future prospective studies with larger study groups are needed.
Self-assessment of the oral hygiene status of children with hemophilia could serve as a basis for the prevention of dental diseases, such as tooth decay and periodontal diseases, and can help prevent complications during dental treatment [12]. The habits of children copy those of their parents, so an evaluation of the family environment is essential. When the parents’ awareness is evaluated, it is easier to understand the oral hygiene practices of the children, too. Oral hygiene knowledge and practices directed toward children with coagulopathies through educational programs could be maintained through the whole life, staring from an early age. With basic guidance, motivation, and preventive care by primary dental professionals, it would be easier for the children to become autonomous in their daily activities [13].
Therefore, this case control study aimed to evaluate the oral hygiene awareness and habits of 31 children aged between 6 to 18 years with hemophilia in Bulgaria.
Material and Methods
DESIGN:
This case control study was conducted in Bulgaria over a 4-year period, from 2017 to 2020. Data was collected from 139 children, of which 31 had hemophilia and 108 did not. Children from the control group were matched with the those in the hemophilia group based on sex, age, and place of residence [8]. The socio-demographical information about children and parents was collected through self-administered questionnaires, which were developed in the local language, Bulgarian, for self-assessment of their dental hygiene habits. Data were collected from January 2017 to June 2020. The participants evaluated were 31 children with hemophilia, 108 children without hemophilia, and 33 parents of children with hemophilia.
The use of questionnaires provided information about the demographic characteristics of the participants, their knowledge of oral hygiene, oral hygiene habits, and self-assessment of their oral status. Some questions had options for multiple answers.
The study was conducted at the following: a summer camp for parents of children with hemophilia from 0 to 3 years old in Strelcha (Bulgaria), summer rehabilitation camp for children with hemophilia between 7 and 14 years old in Kranevo (Bulgaria), individual and group dental practices, and dental centers in Bulgaria. By means of statistical analysis, children were allocated to 4 age groups and parents to 5, based on age-dependent differences. The education level of the study participants was classified into 4 categories: pre-school, primary (grades 1–4), lower secondary (grades 5–7), and upper secondary (grades 8–12), with an additional undergraduate category for parents (with postgraduate diploma-bachelor or higher degree). The distribution of children with hemophilia by residence in Bulgaria was based on the classification of the Nomenclature of Territorial Units for Statistics, dividing the location of residences into 6 regions. The study protocol was approved by the Commission on Scientific Ethics at the Medical University of Plovdiv, Bulgaria (protocol no. 6/07.10.2021). The data presented for approval included the application form for consideration for ethical expert assessment of scientific research and projects including human subject research, questionnaire forms for the groups of children with and without hemophilia and parents of children with hemophilia, informed consent form for participation in the study from parents regarding their children, declaration of agreement to comply with the Declaration of Helsinki and its principles for medical research involving human subjects, and design and summary of the scientific research.
STATISTICAL ANALYSIS:
Normally distributed variables are presented as mean±standard deviation. Statistical hypothesis tests for difference of means were calculated using the
Results
SOCIO-DEMOGRAPHIC CHARACTERISTICS OF THE GROUPS:
The 31 surveyed children with hemophilia were between 7 and 18 years of age (mean 11.55±0.58) and, owing to the specificity of the disease, were only boys (Table 1). There were 30 children with hemophilia A and 1 with hemophilia B. The children in the control group without hemophilia were aged between 5 and 18 years (mean 12.30±0.30). The largest proportions of respondents were children with primary education (n=13, 41.90±2.95%), which was also influenced by the location of the surveys at the children’s summer camp.
There was no statistically significant difference between level of education and residence by region among the children with hemophilia
DENTAL HABITS:
Children from both groups confirmed that they used a toothbrush and toothpaste in performing oral hygiene procedures (Table 2). The respondents from all groups were aware of adjunctive oral hygiene methods, but not all were familiar with the correct techniques for dental plaque removal. However, there was no significant difference between the groups in methods used for oral hygiene (P>0.05). A high preference for gum chewing was observed in children, whereas none of the adult respondents reported chewing gum. Adults preferred adjunctive methods, such as using toothpicks, which were not used in the group of children with hemophilia. When asked to explain how to use toothpicks, children were unsure. They were usually hesitant to cause gingival bleeding after cleaning the interdental space. Interdental floss was used as an alternative oral hygiene method in about 20% of the respondents from families with hemophilia. Children explained that the interdental brush was easier to operate than interdental floss.
The duration of oral hygiene procedures was about 1 min (n=5, 16.13±6.61%) or 2 min (n=13, 41.94±8.86%), which is considered insufficient for proper oral hygiene (Table 3). There was a smaller proportion of children with hemophilia who brushed their teeth for 3 min or more. Longer toothbrushing duration was associated with other hygiene habits. For example, there was an association between longer toothbrushing and the use of dental fluoride in different forms (χ2=6.64, P<0.05). Children in both groups used fluoride supplements, but children with hemophilia were more likely to consider it as a method for caries prevention.
Frequent oral hygiene habits lead to a significant reduction of anaerobic microorganisms, which cause periodontal diseases in the mouth cavity and create the need to visit the dentist regularly for routine preventive examinations. The proportions of children with and without hemophilia were significantly different in regards to past dental visits (χ2=13.30,
It is important for the long-term outcomes of oral health improvement in children with comorbidities for the dentist to achieve a high degree of cooperation with the children. Receiving professional dental advice was associated with the duration of toothbrushing in children with hemophilia (χ2=6.85, P<0.05). However, most of the patients with hemophilia responded that they had not received any professional help for oral hygiene improvement (n=18, 58.06±8.86%). More than half of the children in the control group were educated about correct oral hygiene techniques by a dental professional (n=68, 62.96±4.65%). In the present study, children who received oral hygiene advice by a dentist brushed their teeth significantly longer (n=9, 69.23±12.80%) than those who had not received advice, which was also found in previous studies [8,9].
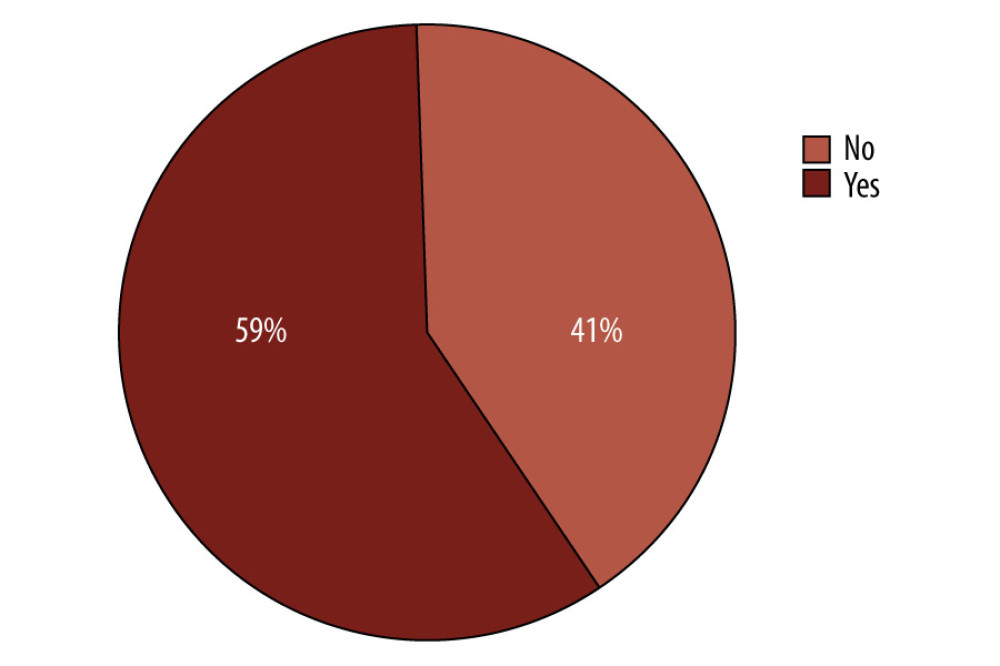
In addition to professional dental motivation in clinics, which was provided periodically, motivation for oral hygiene improvement was associated with family education. Most of the children in both groups had received advice from their parents regarding oral hygiene. Nevertheless, more than half of the children with hemophilia had experienced bleeding episodes from the oral cavity (Figure 1).
Discussion
Several epidemiological studies have been conducted in Bulgaria to register people with coagulopathies, of which there are a total of 610 patients with hemophilia A (7 per 100 000 people) and 85 patients with hemophilia B (0.7 per 100 000 people). Evaluation of the oral status of such patients was based on groups with a small number of patients [14].
The sample size of similar studies included the observation of children only, or both adults and children with hemophilia. In the present study, the focus was to assess only the pediatric population with respect to the habits of the family environment. This study aimed to evaluate and compare the oral hygiene habits among children with hemophilia, their parents, and age-matched controls. Most studies explaining the health behavior of children with hemophilia included boys only, with few including female participants.
In providing quality dental services for people with coagulopathies, despite the macro-economic stability, Bulgaria still strives to attain the EU standards in medical development and oral health policy. Until now, there are no official dental protocols for the treatment of people with bleeding disorders in Bulgaria. There is no published research conducted on the dental status and dental treatment needs of children with hemophilia in Bulgaria. Only after a detailed professional evaluation of the dental needs of children with disabilities can recommendations be implemented in the programs for oral health improvement. However, reducing inequality in the access to primary and specialized medical services and dental care for children with chronic diseases is within the key recommendations of UNICEF, which is among the main medically and socially justified policies, defining the priority in oral health improvement, including for children with hemophilia [15].
The latest active oral health program in Bulgaria including the pediatric population is the National Program for Prophylaxis of Oral Diseases in Children Ages 0 to 18 Years, from 2021–2026, which continues the national program from 2014–2020. In its focus is proper oral hygiene among children with the use of toothbrushes, toothpastes with fluoride, and dental floss. It is the only national and regional activity established regarding the oral hygiene improvement of children. All children and their parents (guardians) should be trained and educated in all basic prophylactic methods. As a result, they should acquire adequate knowledge and skills as part of their value system [16].
After a detailed study and comparison of oral hygiene status in children with and without hemophilia, researchers found conflicting results [8]. Age is associated with the ability of individuals to perform oral hygiene procedures [12–14]. This is because children with hemophilia have a high awareness of the options for prophylaxis as prevention of life-threatening dental conditions. Some authors found poor oral hygiene status in the hemophilia groups (
The same tendency was observed in the frequency of brushing habits between children with hemophilia (n=100, 23%) and a control group (n=100, 46%) in India, with more brushing in the healthy group (
A main principle of dental prevention for people with hemophilia is that everyone should be given the opportunity for self-assessment of the risk factors of early childhood caries. Standard dental prophylaxis is suitable for children with a low risk level of caries, while specific prophylaxis is used in children with an increased caries risk or in those assigned to a category with a high risk owing to other factors (eg, medical conditions) [3]. Teaching patients from an early age about the methods of maintaining personal oral hygiene, such as the correct toothbrushing technique, should be implemented in educational programs for children with hemophilia [4]. Health information and education for risk groups is important because irregular oral hygiene leads to significant bleeding. If toothbrushing causes bleeding, a temporary solution is mouth rinsing after each meal and improvement of the personal hygiene technique. Sufficient oral hygiene reduces the necessity of invasive dental treatment and the number of dental appointments [5,7]. Regular self-assessment and professional assessment of the oral status of families with hemophilia make it possible to evaluate not only the quality of life, but also whether the treatment provided to each patient is appropriate for them.
Educating patients about correct preventive methods has significant health benefits, which are proven over time. Fluoride has been used in dentistry for nearly a century and is considered as an essential protective factor in decreasing tooth decay. However, to achieve the maximum benefit of fluoride prophylaxis, it should be used in combination with different types of methods for personal oral hygiene. No significant difference was found in the fluoride used during oral hygiene or fissure sealant application in the literature [19,20].
Our study found a statistically significant difference between the reasons for dental visits between both groups of children, which was also found by other authors. However, a study in Malaysia found that there was a difference between groups (
Children’s behavior largely matches that of their parents; therefore, the family environment of children with hemophilia is a key to understand and build oral hygiene habits in the young generation. A significant difference in overall oral health has been seen between some groups of children with and without hemophilia. As a result of the positive impact of the family habits implemented in children, the overall dental health of children with hemophilia was evaluated as better than that of children without hemophilia [19]. Although this may partly be explained by genetic factors, environmental factors, such as established preventive dental routines at home, also contribute to this finding. Dental health culture should be extended from an individual to group level so that all family members receive the proper education. In practice, it is difficult for families with hemophilia to implement the recommendations of dental professionals at home. The focus should be in the control of children performing their daily dental routine so that they become autonomous.
Further, incorporating dental care as a part of the specialized hemophilia centers may enhance confidence and acceptance of the dental care and help to decrease the risk of bleeding during dental appointments [21,22].
Even though different national and international protocols and programs have considered dental treatment of children with hemophilia, there are still no strict recommendations or absolute statements in dental guidelines for Bulgaria. It may be because most studies showed diverse attitudes of medical and dental professionals to the treatment approach regarding this topic [23].
Conclusions
The findings of this study of children with hemophilia in Bulgaria support those of previous studies from other countries and support the need to improve oral hygiene practices in this group of patients. Children with hemophilia have a high awareness of oral hygiene methods, but more attention should be focused on additional individually based education at the dental office. More frequent self-assessment of children with hemophilia and further evaluation of their oral hygiene routine could identify the factors compromising the dental status in this vulnerable population.
References
1. Abrisham M, Tabrizizadeh M, Ghateh A, Knowledge of oral hygiene among hemophilic patients referred to Iranian Hemophilia Society: J Dent Res Dent Clin Dent Prospects, 2009; 3(2); 60-63
2. Sheiham A, Oral health, general health and quality of life: Bull World Health Organ, 2005; 83(9); 641-720
3. Anderson JA, Brewer A, Creagh D, Guidance on the dental management of patients with haemophilia and congenital bleeding disorders: Br Dent J, 2013; 215(10); 497-504
4. Rizza CR, Matthews JM, Management of the haemophilic child: Arch Dis Child, 1972; 47(253); 451-62
5. Kumar JN, Kumar RA, Varadarajan R, Sharma N, Specialty dentistry for the hemophiliac: Is there a protocol in place?: Indian J Dent Res, 2007; 18; 48-54
6. Jangra B, Goswami M, Assessment of dental caries experience and periodontal health status among children with haemophilia in New Delhi, India – a case control study: Oral Health Prev Dent, 2017; 15(2); 131-37
7. Gómez-Moreno G, Cañete-Sánchez ME, Guardia J, Orthodontic management in patients with haemophilia. About two clinical cases: Med Oral Patol Oral Cir Bucal, 2010; 15(3); e463-66
8. Žaliūnienė R, Aleksejūnienė J, Brukienė V, Pečiulienė V, Do hemophiliacs have a higher risk for dental caries than the general population?: Medicina (Kaunas), 2015; 51(1); 46-56
9. Salem K, Eshghi P, Dental health and oral health-related quality of life in children with congenital bleeding disorders: Haemophilia, 2013; 19(1); 65-70
10. Reddy KS, Reddy NV, Niharika P, Reddy MA, Oral health status and treatment needs among hemophilic children in hyderabad, Telangana, India: Int J Clin Pediatr Dent, 2019; 12(1); 30-32
11. Kanjani V, Annigeri RG, Hanagavadi S, Manjunath MR, Comparative analysis of oral health and treatment necessities in hemophilia individuals of Davangere population – a case control study: J Family Med Prim Care, 2020; 9(9); 4774-77
12. Gaddam KR, Nuvvula S, Nirmala S, Kamatham R, Oral health status among 6- to 12-year-old haemophilic children – an educational intervention study: Haemophilia, 2014; 20(4); e338-41
13. Huang J, Yao Y, Jiang J, Li C, Effects of motivational methods on oral hygiene of orthodontic patients: A systematic review and meta-analysis: Medicine (Baltimore), 2018; 97(47); e13182
14. Kumar M, Pai KM, Kurien A, Vineetha R, Oral hygiene and dentition status in children and adults with hemophilia: A case-control study: Spec Care Dentist, 2018; 38(6); 391-94
15. UNICEF: Situation analysis of children and women in Bulgaria, 2018, UNICEF Available from: https://www.unicef.org/bulgaria/media/2821/file/BGR-situation-analysis-childrenwomen-bulgaria.pdf
16. : National program for prevention of oral diseases in children from 0 to 18 years in Republic of Bulgaria for the period 2015–2020 Available from:https://www.oralnaprofilaktika.bg/Nationalna_%20programa_oralni_zaboliavania.pdf
17. Othman NAA, Sockalingam SNM, Mahyuddin A, Oral health status in children and adolescents with haemophilia: Haemophilia, 2015; 21(5); 605-11
18. Parvaie P, Shaygan MH, Ziaee M, Evaluation of gum health status in hemophilia patients in Birjand (a case-control study): Am J Blood Res, 2020; 10(3); 54-59
19. Kabil N, ElAlfy MS, Metwalli N, Evaluation of the oral health situation of a group of Egyptian haemophilic children and their re-evaluation following an oral hygiene and diet education programme: Haemophilia, 2007; 13(3); 287-92 [Erratum in: Haemophilia. 2011;17(6):979]
20. Buzalaf MAR, Pessan JP, Honório HM, Ten Cate JM, Mechanisms of action of fluoride for caries control: Monogr Oral Sci, 2011; 22; 97-114
21. Jangra B, Goswami M, Assessment of dental caries experience and periodontal health status among children with haemophilia in New Delhi, India – a case control study: Oral Health Prev Dent, 2017; 15(2); 131-37
22. Rajantie H, Alapulli H, Mäkipernaa A, Ranta S, Oral health care in children with haemophilia in Helsinki, Finland: Eur Arch Paediatr Dent, 2013; 14(5); 339-43
23. Bajkin B, Dougall A, Current state of play regarding dental extractions in patients with haemophilia: Consensus or evidence-based practice? A review of the literature: Haemophilia, 2020; 26(2); 183-99
Tables
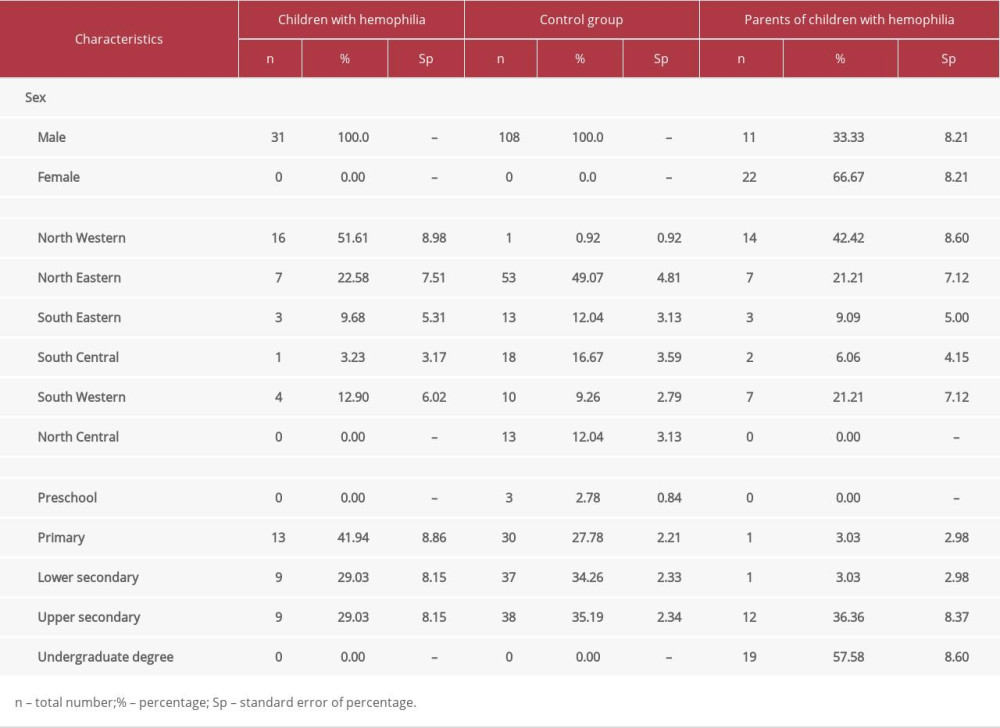 Table 1. Socio-demographic characteristics of study participants.
Table 1. Socio-demographic characteristics of study participants.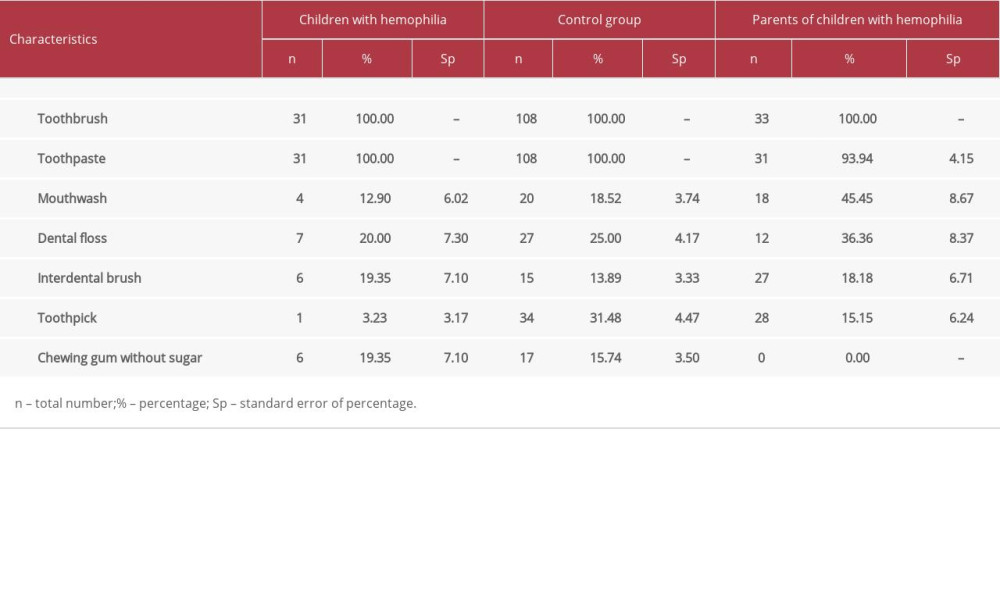 Table 2. Methods of oral hygiene.
Table 2. Methods of oral hygiene.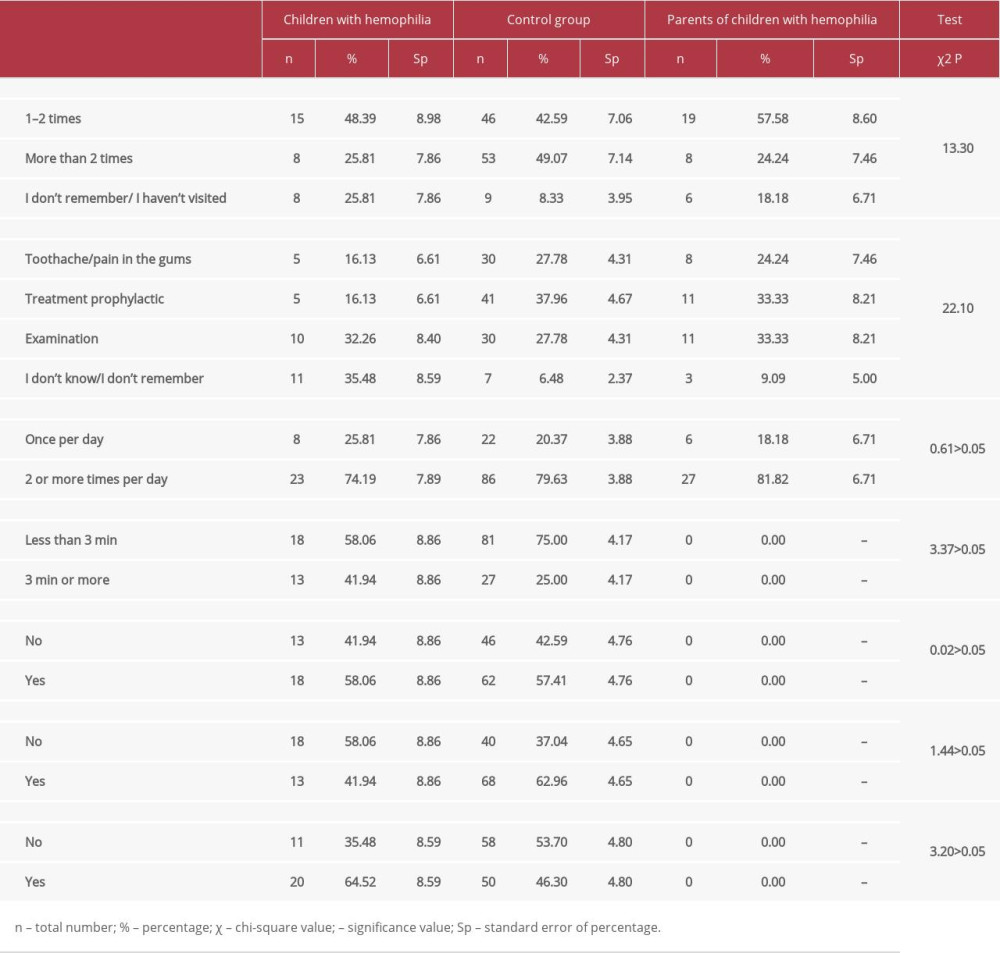 Table 3. Oral-health related awareness among children with hemophilia and parents.Table 1. Socio-demographic characteristics of study participants.Table 2. Methods of oral hygiene.Table 3. Oral-health related awareness among children with hemophilia and parents.
Table 3. Oral-health related awareness among children with hemophilia and parents.Table 1. Socio-demographic characteristics of study participants.Table 2. Methods of oral hygiene.Table 3. Oral-health related awareness among children with hemophilia and parents. Most Viewed Current Articles
13 Apr 2020 : Original article 19,586
Outcome of 24 Weeks of Combined Schroth and Pilates Exercises on Cobb Angle, Angle of Trunk Rotation, Chest...DOI :10.12659/MSMBR.920449
Med Sci Monit Basic Res 2020; 26:e920449
20 Apr 2018 : Original article 17,466
Brain Training Games Enhance Cognitive Function in Healthy SubjectsDOI :10.12659/MSMBR.909022
Med Sci Monit Basic Res 2018; 24:63-69
23 Jul 2016 : Review article 10,353
Cardiac Hypertrophy: An Introduction to Molecular and Cellular BasisDOI :10.12659/MSMBR.900437
Med Sci Monit Basic Res 2016; 22:75-79
10 Aug 2020 : Clinical Research 9,788
Effects of Cognitive Task Training on Dynamic Balance and Gait of Patients with Stroke: A Preliminary Rando...DOI :10.12659/MSMBR.925264
Med Sci Monit Basic Res 2020; 26:e925264