27 October 2021: Clinical Research
Accuracy of Continuous and Noninvasive Hemoglobin Monitoring in the Presence of CO Insufflation: An Observational Pilot Study
Hye Sun LeeDOI: 10.12659/MSM.933027
Med Sci Monit 2021; 27:e933027






Abstract
BACKGROUND: Laparoscopic surgery has several benefits, but it requires prolonged carbon dioxide (CO₂) insufflation. Several factors affect the accuracy of continuous and noninvasive hemoglobin (SpHb) monitoring, but the effects of CO₂ insufflation are undetermined. This study investigated the effect of CO₂ insufflation on SpHb monitoring in laparoscopic surgery.
MATERIAL AND METHODS: Twenty patients undergoing laparoscopic gastrectomy were enrolled. Anesthesia was maintained using sevoflurane and remifentanil within an end-tidal CO₂ of 30-45 mmHg. The CO₂ insufflation was maintained at 12 mmHg using CO₂. SpHb was monitored with a Radical-7 Pulse CO-Oximeter, and laboratory hemoglobin (tHb) was analyzed using a satellite blood analyzer.
RESULTS: Forty paired measurements were analyzed. The mean perfusion index, SpHb, and tHb were 3.10±1.77%, 10.92±1.48 g/dL, and 11.51±0.88 g/dL, respectively. SpHb underestimated tHb with a bias (precision) of -0.59 (1.28 g/dL), and the 95% limit of agreement was wide (-3.11 to 1.92 g/dL). SpHb was moderately correlated with tHb (r=0.50, 95% CI: 0.23 to 0.70). The concordance rate was 67%. ΔSpHb was not correlated with ΔtHb (r=0.29, 95% CI: -0.18 to -0.65). A similar bias, wider limits of agreement, a higher |SpHb-tHb|, but more significant correlation between SpHb and tHb were observed for the “PaCO2 <40 mmHg” range compared with the “40 mmHg ≤PaCO₂” range.
CONCLUSIONS: SpHb may have an acceptable accuracy but has a weak trending ability in the presence of CO₂ insufflation, and it can be affected by PaCO₂. Further research on the effects of CO₂ insufflation on SpHb is needed.
Keywords: Hemoglobins, Laparoscopy, Monitoring, Intraoperative, Pneumoperitoneum, Carbon Dioxide, Female, Humans, Insufflation, Male, Pilot Projects
Background
Minimally invasive surgeries, such as laparoscopic and robotic surgeries, have become increasingly common due to their advantages, including less intraoperative bleeding, faster recovery, shorter hospitalization, and improved quality of life compared to open surgery [1]. However, it requires prolonged carbon dioxide (CO2) insufflation, which causes physiologic changes related to hypercarbia and respiratory acidosis [2].
Continuous and noninvasive hemoglobin (SpHb) monitoring using a Radical-7 Pulse CO-Oximeter displays the blood hemoglobin (Hb) concentrations on a monitor using a spectrophotometric Hb sensor. SpHb monitoring is based on the measurement of the differential optical density of light at multiple wavelengths that pass through the tissue. SpHb allows clinicians to rapidly detect occult bleeding and effectively perform transfusion without blood loss due to repeated blood draws [3]. Its usefulness perioperatively [3] and in traumatized patients with low Hb levels has been documented [4]. A meta-analysis reported an acceptable accuracy of SpHb based on 28 studies conducted only in the operating room [5]; subgroup analysis was performed for age, continent, method (venous or arterial), funding, and measurements (single or multiple), but no subgroup was based on CO2 insufflation.
In a previous study, the altered arterial CO2 pressure (PaCO2) levels reduced the agreement between arterial oxygen saturation measured by pulse oximetry and arterial oxygen pressure (PaO2) as calculated from arterial blood gas co-oximetry [6]. Moreover, increased end-tidal CO2 tension (EtCO2) enhances regional cerebral oxygen saturation in obese patients during laparoscopic surgery [7]. Although there have been no experimental studies regarding the effect of PaCO2 on oximetry, an increased carbaminohemoglobin level and changes in red blood cell morphology was proposed as a mechanism [6].
SpHb is affected by several factors, such as laboratory hemoglobin concentration (tHb), perfusion index (PI), hemodilution during fluid loading, dark skin, and indigo carmine [8–12]; however, it has not yet been determined whether the elevated PaCO2 in the presence of CO2 insufflation affects the agreement between SpHb and invasive tHb. Therefore, this observational pilot study aimed to investigate the accuracy of SpHb in the presence of CO2 insufflation in patients undergoing laparoscopic surgery.
Material and Methods
PATIENT RECRUITMENT:
This prospective observational pilot study involved patients undergoing laparoscopic gastrectomy between November 2017 and December 2017 at Ajou Hospital, Suwon, Republic of Korea. The study protocol was approved by the Ajou University Hospital Institutional Review Board (IRB number: AJIRB-MED-OBS-17-216) and registered with
ANESTHESIA:
On arrival in the operating room, standard monitoring including pulse oximetry, electrocardiography, bispectral index, and noninvasive blood pressure measurements were performed. General anesthesia was induced with intravenous propofol (2.0 mg/kg) and remifentanil (3.0–4.0 ng/mL as target concentrations) using target-controlled infusion. Rocuronium bromide (1 mg/kg) was used to facilitate orotracheal intubation. A 20-G radial arterial catheter was inserted for continuous monitoring of hemodynamics and blood sampling. Mechanical ventilation was used to maintain EtCO2 between 30 and 45 mmHg with 50% inspired oxygen with air. Anesthesia was maintained with continuous infusion of remifentanil (0–5.0 ng/mL) and sevoflurane at 2 vol% to achieve a bispectral index value of 40–60 and a mean arterial pressure (MAP) within 20% of the baseline. Rocuronium (0.2–0.4 mg/kg/h) was also continuously infused. Lactate Ringer’s solution with 6% hydroxyethyl starch solution (Volulyte, Fresenius Kabi, Bad Homberg, Germany) was infused at a constant rate of 6 mL/kg/h. In the case of MAP of <60 mmHg, an intravenous bolus of ephedrine (4 mg) was administered. At the end of the surgery, the neuromuscular block was reversed using sugammadex (2 mg/kg), and tracheal extubation was performed.
All procedures were performed by 3 skilled surgeons using the same method. The reverse Trendelenburg positioning was performed at 30° until the removal of endoscopy. The abdominal insufflation was formed using CO2, and the abdominal gas pressure was set at 12 mmHg in all patients.
SPHB AND THB MEASUREMENTS:
Before the induction of anesthesia, an adult disposable spectrophotometric Hb sensor (Rainbow R1 25, Rev E; Masimo, Irvine, CA, USA) was applied to the fourth finger of the patient and was covered with an impermeable black shield to prevent optical interference (by N.Y.K). SpHb levels were continuously monitored using a Radical-7 Pulse CO-Oximeter (software version 1451; Masimo Corporation, Irvine, CA, USA).
For tHb, the blood sample was taken from the arterial catheter, and then sample was analyzed immediately after collection with an operation room satellite blood analyzer (Stat Profile pHOx Ultra; Nova Biomedical, Waltham, MA, USA). Blood sampling were performed at 2 time points: 60 min after the CO2 insufflation and 10 min before the end of surgery (by H.Y.K. and N.Y.K.). Simultaneously, SpHb values were recorded within 10 s after blood sampling. In vivo adjustment (calibration) was not performed.
The blood gas was calculated for pH, PaCO2, PaO2, tHb, and bicarbonate. Data on the monitor including EtCO2 and hemodynamics (heart rate and MAP) also were recorded simultaneously with the SpHb recording. PI, a measure of peripheral circulation calculated by the Pulse CO-Oximeter, was also recorded at the time of the blood draw. All PI values <1.0 were included.
STATISTICAL ANALYSIS:
The values are reported as mean±standard deviation (SD), median (interquartile range), or number (%). The normality of the distribution was assessed using the Shapiro-Wilk test. All paired data (SpHb-tHb) and changes in SpHb (ΔSpHb) and tHb (ΔtHb) between the 2 consecutive measurements were analyzed. The statistical analyses were performed using SPSS for Windows (version 25.0; IBM Corp., Armonk, NY, USA) and SAS (version 9.4; SAS Inc., Cary, NC, USA).
The Bland-Altman analysis accounting for repeated measurements from the same subject was used to evaluate the agreement and precision between the SpHb and tHb. The bias was derived as SpHb-tHb. The precision was defined as 1 SD of the bias. The 95% limit of agreement (LOA) was calculated as the interval defined by the bias±1.96 SD.
Error grid analysis was used to graphically demonstrate the clinical implications of the differences between SpHb and tHb using an Hb cutoff of 9 g/dL [13]. The value of ±10% was chosen because this deviation represents 1 g/dL Hb at the upper range of transfusion consideration (10 g/dL). The error grid had 3 zones based on the difference between SpHb and tHb (Zones A, B, and C). Zone A had 3 sections according to the Hb value: an isthmus section representing a 10% error for Hb values between 6 g/dL and 10 g/dL, where a transfusion decision may occur, the lowermost section of <6 g/dL where a transfusion will likely occur, and the uppermost section of >10 g/dL where a transfusion is unlikely. Zone B reflects a potential therapeutic error that is not as significant as that of zone C. Zone C represents the potential for a major therapeutic error in the administration of blood. In this analysis, the coefficients of determination (r values) were also calculated.
A 4-quadrant plot was used to demonstrate the trending ability over time with differences in ΔSpHb and ΔtHb [14]. A central exclusion zone of 1 g/dL, approximately 10% of the measured data, was applied to prevent larger random errors. The concordance rate was defined as the percentage of the data points that fell into the quadrants agreement (upper right and lower left), indicating agreement in the direction of change. This was considered a reliable trending ability of more than 90%.
Lastly, for the comparison of groups based on PaCO2, the accuracy-related variables, including bias, LOA, correlation, and the absolute difference between SpHb and tHb, were analyzed with a mixed-effects model for the various PaCO2 ranges (PaCO2 <40 mmHg and PaCO2 ≥40 mmHg).
Results
Of the 31 patients, 11 were excluded, and 20 patients were included, as shown in Figure 1. The patient characteristics and operational data are summarized in Table 1. None of the patients received transfusion during surgery.
Heart rate and MAP were adequately maintained during surgery (Table 2). In arterial blood gas analysis, pH and bicarbonate levels were within the normal range, and PaO2 was maintained at approximately 200 mmHg. The mean PaCO2 values during surgery were 41.58±3.24 (range, 28–47) mmHg.
In total, 40 paired measurements of SpHb and tHb from 20 patients were analyzed. Among them, 4 SpHb measurements were measured with a PI value of <1.0. The mean PI value for the 40 SpHb measurements was 3.10±1.77% (range, 0.5–6.8%). The mean SpHb was 10.92±1.48 g/dL, and the mean tHb was 11.51±0.88 g/dL. Fifteen instances (38%) of all the pairs showed an absolute difference of ≤1.0 g/dL between SpHb and tHb, and 26 instances (65%) showed an absolute difference of ≤1.5 g/dL (Table 3).
An error grid analysis for the data points of all the SpHb and tHb pairs is shown in Figure 2. For all the pairs, 90% (36 of 40) were in zone A and 10% (4 of 40) were in zone B. There were no cases in zone C. In addition, there was a moderate positive correlation between SpHb and tHb: the correlation coefficient (
Bias was similar across the PaCO2 ranges (
Discussion
In this prospective observational pilot study, we evaluated the accuracy of SpHb during laparoscopic surgery. In the presence of CO2 insufflation, the average SpHb tended to underestimate the tHb on consideration of −0.59 (1.28 g/dL) of bias (precision) values. In addition, there was a moderate positive correlation between SpHb and tHb, but no correlation between ΔSpHb and ΔtHb. The group comparison based on the PaCO2 ranges showed conflicting results of bias, a wider LOA, and a higher value of |SpHb-tHb|, but a more significant correlation between SpHb and tHb in the PaCO2 <40 mmHg range.
In our study, the bias (precision) was −0.59 (1.28 g/dL), and the 95% LOA was −3.11 to1.92 g/dL in the presence of CO2 insufflation. A meta-analysis by Kim et al included 32 studies, but only 13 studies were performed in the operating room [15]. Despite the minimal bias and SD of 0.39±1.32 g/dL for the SpHb and tHb, 16 studies in the operation room showed a wide LOA of −2.21 to 2.98 g/dL, and they were not homogeneous (
The error grid analysis showed that SpHb was significantly correlated with tHb in our study (
In the 4-quadrant plot, the concordance had an unacceptable rate of 67%, and ΔSpHb was not correlated with ΔtHb (
The group comparisons based on the PaCO2 ranges showed that PaCO2 can affect the accuracy of SpHb, but the results were inconsistent in our study. In patients with hypercapnia, the PaCO2 status impaired the agreement between PaO2 and arterial oxygen saturation measured by pulse oximetry [6]. In 70 adults undergoing laparoscopic herniorrhaphy, gastric bypass, or cholecystectomy, significant changes in cerebral oxygenation occurred during insufflation during laparoscopy [24]. In laparoscopic bariatric surgery, increased EtCO2 enhances regional cerebral oxygen saturation [7]. As possible mechanism, Munoz et al proposed an increased carbaminohemoglobin level, changes in red blood cell morphology, and venous blood pulsatility [6]. Further experimental studies are needed to determine the effect of PaCO2 on oximetry.
This study has limitations. First, this was a pilot study involving a small sample size, and the statistical power might be too weak to draw definitive conclusions. Second, the baseline values of SpHb and tHb were not measured. Anesthetic drugs can influence the microcirculation and accuracy of SpHb; thus, baseline values obtained after anesthetic induction are needed [25]. Third, a radial arterial catheter was placed on the same side arm as the spectrophotometric Hb sensor. Although radial blood flow decreased immediately and recovered 5 min after cannulation, blood flow reduction at the fingertip may have occurred because the diameters of the radial artery or its dorsal branch significantly decreased after cannulation [26,27]. Fourth, SpHb with PI of <1.0 should be excluded from the final analysis because the decrease in PI after phenylephrine administration reduced the changes in the bias values after anesthesia induction [9].
The results of this study were inconsistent. However, our observation may be meaningful, because the importance of a pilot study with a small sample is to provide estimates for sample size calculation and assist in planning and improving the quality of further research and minimizing unnecessary effort from researchers and participants [28].
Conclusions
This observational pilot study suggests that SpHb has an acceptable accuracy but weak trending ability in the presence of CO2 insufflation, and SpHb may be affected by PaCO2 levels. Further research with larger populations or randomized controlled studies are needed to definitively establish the effect of CO2 insufflation on the accuracy of SpHb.
Figures
 Figure 1. Flow diagram for patient enrollment.
Figure 1. Flow diagram for patient enrollment. 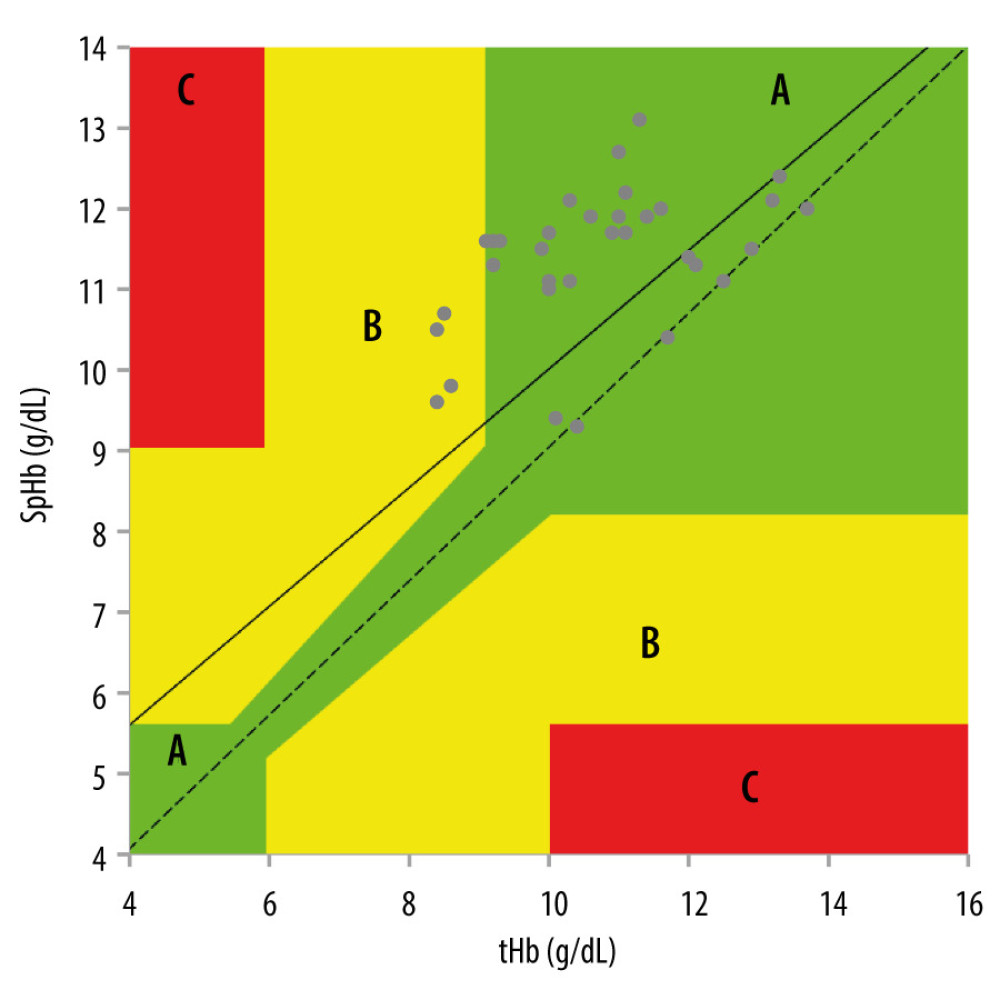 Figure 2. Error grid analysis for the data points of the SpHb and tHb pairs. Zone A represents a clinically acceptable difference (±10%) for hemoglobin from 6 g/dL to 10 g/dL. Zone B represents differences greater than ±10% with a potential for therapeutic error. Zone C represents differences with a major therapeutic error. SpHb – continuous and noninvasive hemoglobin monitoring; tH – laboratory hemoglobin
Figure 2. Error grid analysis for the data points of the SpHb and tHb pairs. Zone A represents a clinically acceptable difference (±10%) for hemoglobin from 6 g/dL to 10 g/dL. Zone B represents differences greater than ±10% with a potential for therapeutic error. Zone C represents differences with a major therapeutic error. SpHb – continuous and noninvasive hemoglobin monitoring; tH – laboratory hemoglobin 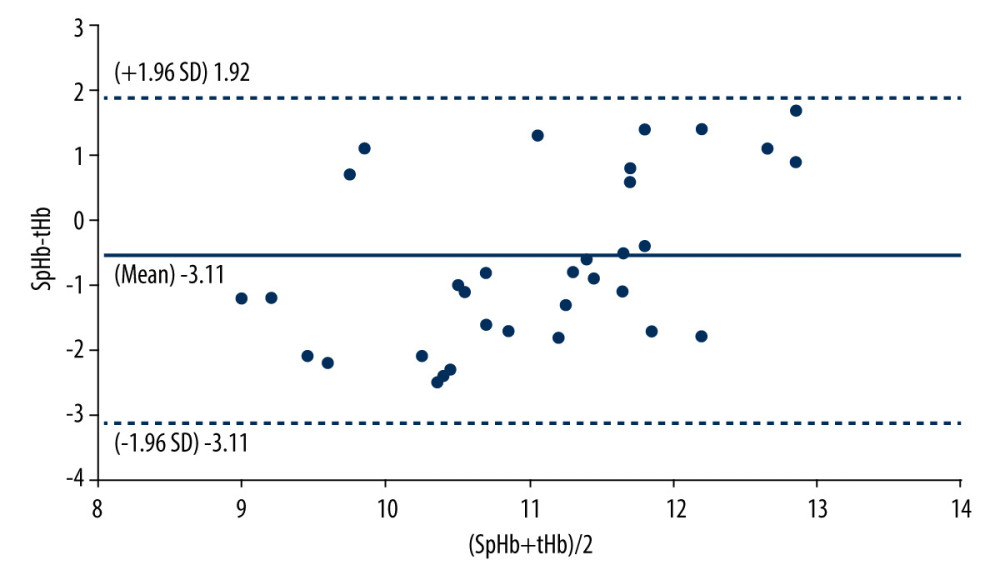 Figure 3. Bland-Altman analysis. The solid line represents the bias (SpHb–tHb), and the dotted line represents the 95% limit of agreement. SpHb – continuous and noninvasive hemoglobin monitoring; tHb – laboratory hemoglobin.
Figure 3. Bland-Altman analysis. The solid line represents the bias (SpHb–tHb), and the dotted line represents the 95% limit of agreement. SpHb – continuous and noninvasive hemoglobin monitoring; tHb – laboratory hemoglobin. 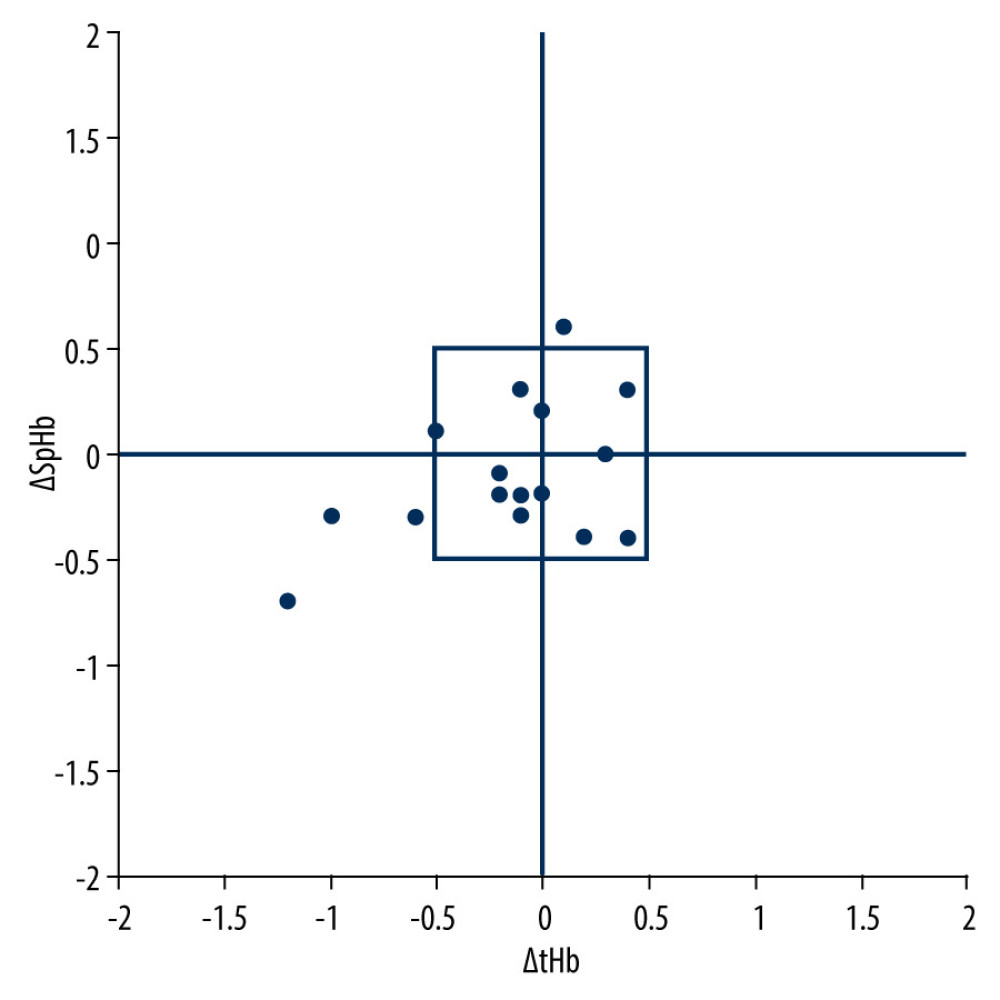 Figure 4. The 4-quadrant plot. It shows the directionality of the trend with a central exclusion zone of 1 g/dL hemoglobin. SpHb – continuous and noninvasive hemoglobin monitoring; tHb – laboratory hemoglobin
Figure 4. The 4-quadrant plot. It shows the directionality of the trend with a central exclusion zone of 1 g/dL hemoglobin. SpHb – continuous and noninvasive hemoglobin monitoring; tHb – laboratory hemoglobin Tables
Table 1. Patient’s characteristics and operational data.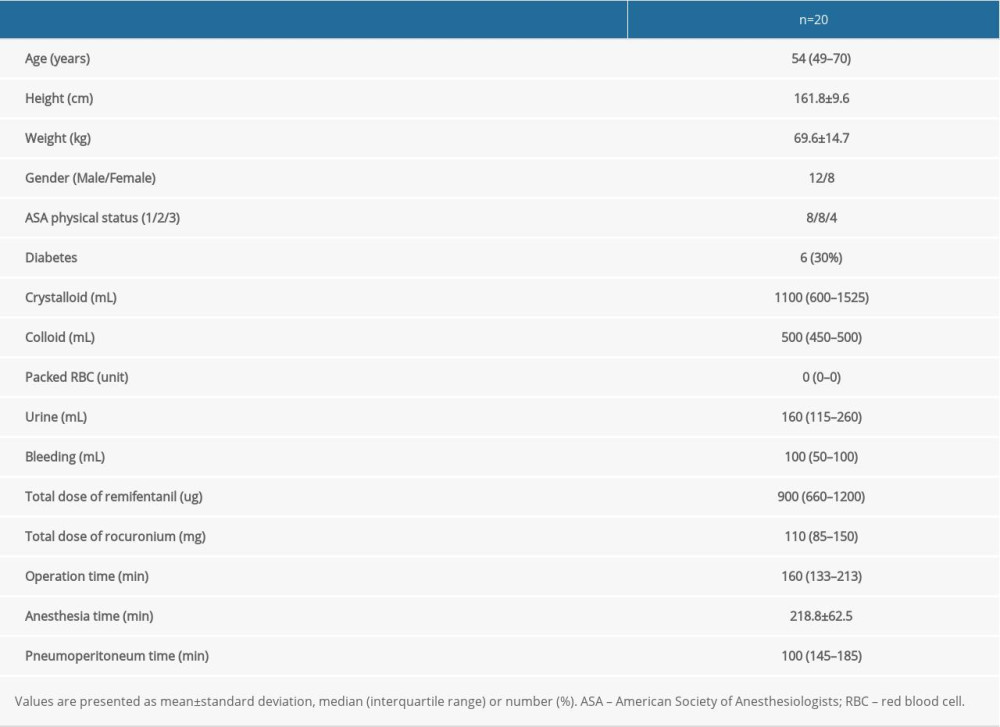 Table 2. Hemodynamics and arterial blood gas analysis.
Table 2. Hemodynamics and arterial blood gas analysis.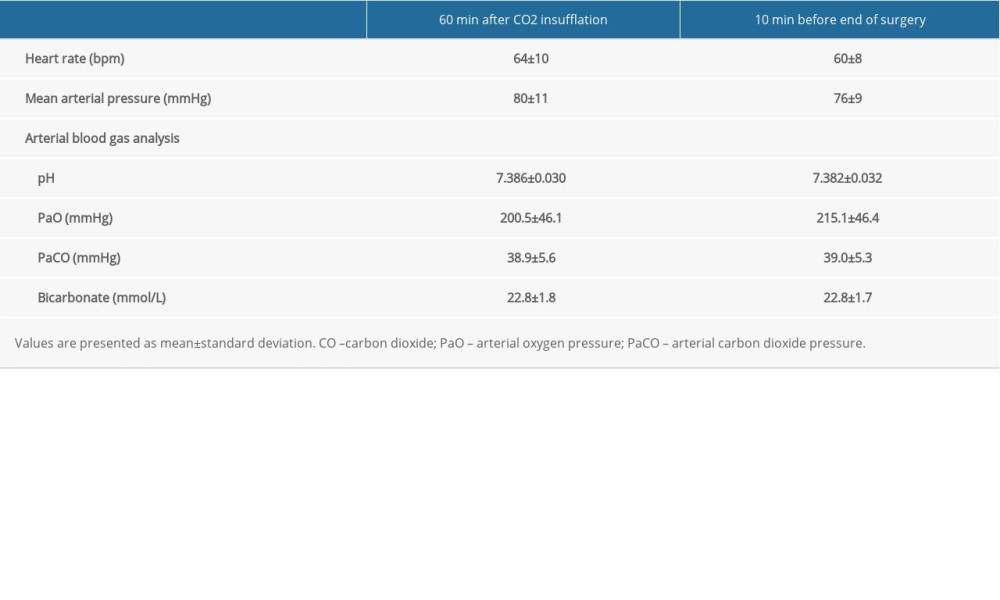 Table 3. Groups based on magnitude of differences between Radical-7 Pulse CO-Oximeter (SpHb) and laboratory CO-Oximeter (tHb) hemoglobin concentration.
Table 3. Groups based on magnitude of differences between Radical-7 Pulse CO-Oximeter (SpHb) and laboratory CO-Oximeter (tHb) hemoglobin concentration. Table 4. Accuracy of SpHb by PaCO2 range.
Table 4. Accuracy of SpHb by PaCO2 range.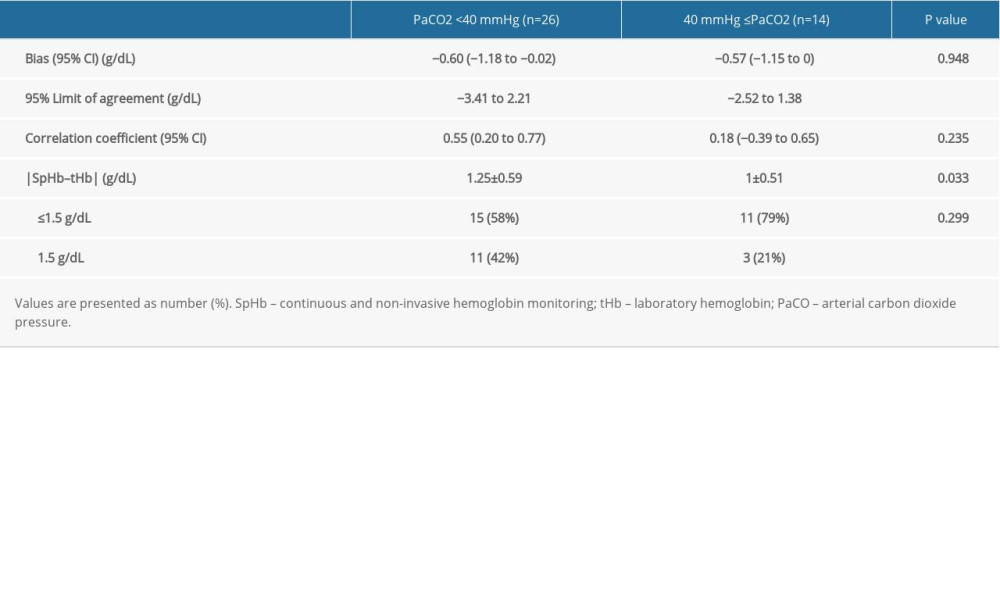
References
1. Costantino CL, Mullen JT, Minimally invasive gastric cancer surgery: Surg Oncol Clin N Am, 2019; 28; 201-13
2. Liu Y, Wang M, Zhu Y, Chen J, Effect of carbon dioxide pneumoperitoneum on acid-base balance during laparoscopic inguinal hernia repair: A prospective randomized controlled study: Hernia, 2020 [Online ahead of print]
3. Barker SJ, Shander A, Ramsay MA, Continuous noninvasive hemoglobin monitoring: A measured response to a critical review: Anesth Analg, 2016; 122; 565-72
4. Baulig W, Seifert B, Spahn DR, Theusinger OM, Accuracy of non-invasive continuous total hemoglobin measurement by Pulse CO-Oximetry in severe traumatized and surgical bleeding patients: J Clin Monit Comput, 2017; 31; 177-85
5. Shabaninejad H, Ghadimi N, Sayehmiri K, Comparison of invasive and noninvasive blood hemoglobin measurement in the operating room: A systematic review and meta-analysis: J Anesth, 2019; 33; 441-53
6. Muñoz X, Torres F, Sampol G, Accuracy and reliability of pulse oximetry at different arterial carbon dioxide pressure levels: Eur Respir J, 2008; 32; 1053-59
7. Asaad OM, Different ventilation techniques and hemodynamic optimization to maintain regional cerebral oxygen saturation (rScO(2)) during laparoscopic bariatric surgery: A prospective randomized interventional study: J Anesth, 2018; 32; 394-402
8. Saito J, Kitayama M, Oishi M, The accuracy of non-invasively continuous total hemoglobin measurement by pulse CO-Oximetry undergoing acute normovolemic hemodilution and reinfusion of autologous blood: J Anesth, 2015; 29; 29-34
9. Saito J, Kitayama M, Amanai E, Impact of acute changes in perfusion index and blood pressure on the accuracy of non-invasive continuous hemoglobin concentration measurements during induction of anesthesia: J Anesth, 2017; 31; 193-97
10. Bubenek-Turconi Ş I, Văleanu L, Popescu M, Continuous noninvasive hemoglobin monitoring reflects the development of acute hemodilution after consecutive fluid challenges: Anesth Analg, 2020; 130; 696-703
11. Murphy SM, Omar S, The clinical utility of noninvasive pulse co-oximetry hemoglobin measurements in dark-skinned critically ill patients: Anesth Analg, 2018; 126; 1519-26
12. Isosu T, Obara S, Hakozaki T, Effects of indigo carmine intravenous injection on noninvasive and continuous total hemoglobin measurement with using the Revision L sensor: J Clin Monit Comput, 2017; 31; 485-86
13. Morey TE, Gravenstein N, Rice MJ, Let’s think clinically instead of mathematically about device accuracy: Anesth Analg, 2011; 113; 89-91
14. Critchley LA, Lee A, Ho AM, A critical review of the ability of continuous cardiac output monitors to measure trends in cardiac output: Anesth Analg, 2010; 111; 1180-92
15. Kim SH, Lilot M, Murphy LS, Accuracy of continuous noninvasive hemoglobin monitoring: A systematic review and meta-analysis: Anesth Analg, 2014; 119; 332-46
16. Schäfer M, Lauper M, Krähenbühl L, A nation’s experience of bleeding complications during laparoscopy: Am J Surg, 2000; 180; 73-77
17. Vos JJ, Kalmar AF, Struys MM, Accuracy of non-invasive measurement of haemoglobin concentration by pulse co-oximetry during steady-state and dynamic conditions in liver surgery: Br J Anaesth, 2012; 109; 522-28
18. American Society of Anesthesiologists Task Force on Perioperative Blood Transfusion and Adjuvant Therapies, Practice guidelines for perioperative blood transfusion and adjuvant therapies: An updated report by the American Society of Anesthesiologists Task Force on Perioperative Blood Transfusion and Adjuvant Therapies: Anesthesiology, 2006; 105; 198-208
19. American Society of Anesthesiologists Task Force on Perioperative Blood Management, Practice guidelines for perioperative blood management: An updated report by the American Society of Anesthesiologists Task Force on Perioperative Blood Management: Anesthesiology, 2015; 122; 241-75
20. Adel A, Awada W, Abdelhamid B, Accuracy and trending of non-invasive hemoglobin measurement during different volume and perfusion statuses: J Clin Monit Comput, 2018; 32; 1025-31
21. Tang B, Yu X, Xu L, Continuous noninvasive hemoglobin monitoring estimates timing for detecting anemia better than clinicians: A randomized controlled trial: BMC Anesthesiol, 2019; 19; 80
22. Awada WN, Mohmoued MF, Radwan TM, Continuous and noninvasive hemoglobin monitoring reduces red blood cell transfusion during neurosurgery: A prospective cohort study: J Clin Monit Comput, 2015; 29; 733-40
23. Erdogan Kayhan G, Colak YZ, Sanli M, Accuracy of non-invasive hemoglobin monitoring by pulse CO-oximeter during liver transplantation: Minerva Anestesiol, 2017; 83; 485-92
24. Gipson CL, Johnson GA, Fisher R, Changes in cerebral oximetry during peritoneal insufflation for laparoscopic procedures: J Minim Access Surg, 2006; 2; 67-72
25. Kim TK, Cho YJ, Min JJ, Tissue microcirculation measured by vascular occlusion test during anesthesia induction: J Clin Monit Comput, 2016; 30; 41-50
26. Kim SY, Lee JS, Kim WO, Evaluation of radial and ulnar blood flow after radial artery cannulation with 20- and 22-gauge cannulae using duplex Doppler ultrasound: Anaesthesia, 2012; 67; 1138-45
27. Numaguchi A, Adachi YU, Aoki Y, Radial artery cannulation decreases the distal arterial blood flow measured by power Doppler ultrasound: J Clin Monit Comput, 2015; 29; 653-57
28. In J, Introduction of a pilot study: Korean J Anesthesiol, 2017; 70; 601-5
Figures
Figure 1. Flow diagram for patient enrollment.Figure 2. Error grid analysis for the data points of the SpHb and tHb pairs. Zone A represents a clinically acceptable difference (±10%) for hemoglobin from 6 g/dL to 10 g/dL. Zone B represents differences greater than ±10% with a potential for therapeutic error. Zone C represents differences with a major therapeutic error. SpHb – continuous and noninvasive hemoglobin monitoring; tH – laboratory hemoglobinFigure 3. Bland-Altman analysis. The solid line represents the bias (SpHb–tHb), and the dotted line represents the 95% limit of agreement. SpHb – continuous and noninvasive hemoglobin monitoring; tHb – laboratory hemoglobin.Figure 4. The 4-quadrant plot. It shows the directionality of the trend with a central exclusion zone of 1 g/dL hemoglobin. SpHb – continuous and noninvasive hemoglobin monitoring; tHb – laboratory hemoglobin Tables
Table 1. Patient’s characteristics and operational data.Table 2. Hemodynamics and arterial blood gas analysis.Table 3. Groups based on magnitude of differences between Radical-7 Pulse CO-Oximeter (SpHb) and laboratory CO-Oximeter (tHb) hemoglobin concentration.Table 4. Accuracy of SpHb by PaCO2 range.Table 1. Patient’s characteristics and operational data.Table 2. Hemodynamics and arterial blood gas analysis.Table 3. Groups based on magnitude of differences between Radical-7 Pulse CO-Oximeter (SpHb) and laboratory CO-Oximeter (tHb) hemoglobin concentration.Table 4. Accuracy of SpHb by PaCO2 range. In Press
12 Mar 2024 : Clinical Research
Preoperative Blood Transfusion Requirements for Hemorrhoidal Severe Anemia: A Retrospective Study of 128 Pa...Med Sci Monit In Press; DOI: 10.12659/MSM.943126
12 Mar 2024 : Clinical Research
Tissue Inhibitors of Metalloproteinase 1 (TIMP-1) and 3 (TIMP-3) as New Markers of Acute Kidney Injury Afte...Med Sci Monit In Press; DOI: 10.12659/MSM.943500
12 Mar 2024 : Review article
Optimizing Behçet Uveitis Management: A Review of Personalized Immunosuppressive StrategiesMed Sci Monit In Press; DOI: 10.12659/MSM.943240
12 Mar 2024 : Clinical Research
Metabolomic Alterations in Methotrexate Treatment of Moderate-to-Severe PsoriasisMed Sci Monit In Press; DOI: 10.12659/MSM.943360
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952