03 November 2022: Laboratory Research
Evaluation of Antimicrobial Effectiveness of Dental Cement Materials on Growth of Different Bacterial Strains
Zana D. Lila-KrasniqiDOI: 10.12659/MSMBR.937893
Med Sci Monit Basic Res 2022; 28:e937893






Abstract
BACKGROUND: The aim of this study was to evaluate the antimicrobial effectiveness of dental cement materials for the prevention of bacterial growth, which can cause failure of fixed cementation.
MATERIAL AND METHODS: We developed an agar diffusion disk test in-house to evaluate the antibacterial properties of 3 commercially available dental cement materials (Ketac, Harvard FLB, and Panavia SA Universal Dual Resin cements) compared with a negative control. The materials were tested for the inhibition against Streptococcus mutans (ATCC 10449), Streptoccocus salivarius (ATCC 25975), Enterococcus faecalis (ATCC 29212), and Lactobacilus acidophilus (ATCC 4356). The antimicrobial effectiveness of materials was expressed as the diameters of the inhibition zones around the disk.
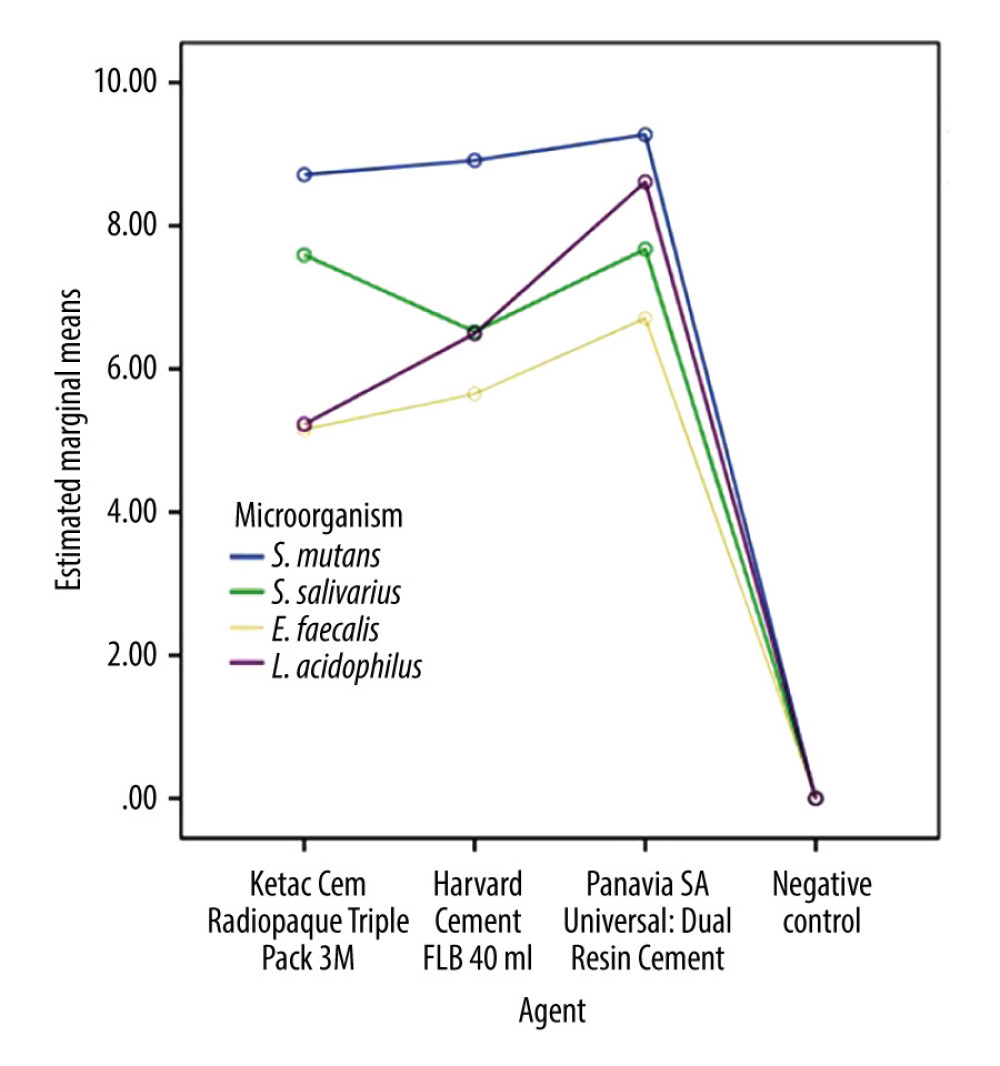
RESULTS: Overall, 240 specimens were tested. All cement materials showed antimicrobial effectiveness. Different microbial strains reacted differently to the different dental cements (all P<0.001). The bacterial strain of S. mutans showed the largest zones of inhibition of all cements, and E. faecalis was less susceptible. Statistically significant differences were observed when comparing different materials among each other (P<0.001). The fluoride-releasing material Panavia was significantly superior to the other 2 materials (P<0.001).
CONCLUSIONS: Fluoride-releasing dental cements showed antimicrobial properties, showing resin cements having superior antimicrobial effects when compared with conventional glass ionomer or zinc phosphate cements.
Keywords: Dental Caries, Dental Cements, Anti-Infective Agents, Anti-Bacterial Agents, Streptococcus mutans, Resin Cements
Background
Dental cement materials are used in fixed prosthodontics and act as luting agents for dental crowns and bridges to natural teeth or implants [1]. Therefore, retention of fixed partial dentures relies on the adaptation of prosthetic material to the tooth surface by the dental cement material. To cement the crown to the tooth, there is a space left between the crown and tooth, called the “cement gap”. This gap is the main reason for failed cementation, as the margin can ensure the environment for colonization of microorganisms, which can create bacterial biofilm and cause periodontitis, periimplantitis, and secondary caries [2–4]. Owing to the different sources of dental cements, previous studies investigated not only their chemical composition, physical properties, and application, but also their antimicrobial effectiveness [5]. Resolving antimicrobial effectiveness led to a range of solutions, including minimizing the cement gap, improving oral hygiene, developing dental cement that is less susceptible for adherence of bacteria and thus biofilm development, and, finally, developing cements that have an antimicrobial effect [6–9]. Studies showed differences in antimicrobial effects, and there is no consensus on which material shows superiority in this matter [10–14].
To date, zinc phosphate is the material that has been most widely used for luting. It has a low solubility; however, the retention relies entirely on mechanical retention. Zinc polycarboxylate cement, by contrast, shows proper adhesion due to the chemical interaction with enamel and stainless steel. However, its solubility is relatively high, which can be considered a disadvantage [15]. Therefore, glass ionomer cements have become more popular as luting and cementation agents [16]. Glass ionomer cements have lower solubility in saliva, have higher strength for compression, and form ionic bonds with stainless steel in prosthetic materials [15]. However, the key disadvantages of glass ionomer cement are the sensitivity to moisture during its setting and time limitation to achieve maximum bond strength [16,17]. Next, resin-modified glass ionomer was developed as an advanced glass ionomer hybrid material with the intention to preserve low solubility, the ability to chelate via the acid–base reaction to enamel and metal, moisture tolerance, and high strength. The potential limitation of this material is its questionable fluoride release [16,18].
The evolution is clearly seen in the development of cements. In addition to all mentioned properties, such as high retention, strength, and easy removal, an ideal dental cement material should also inhibit the development of bacterial plaques [19]. For instance, secondary caries with the formation of bacterial biofilm is the main reason for failed fixed partial dentures. Secondary caries occur due to the colonization of bacteria at locations with low oxygen. Cariogenic bacteria such as
Material and Methods
BACTERIAL SAMPLES:
The antimicrobial performance of cement materials was tested against
CREATION OF DISK DIFFUSION ASSAY AND ANTIMICROBIAL TESTING:
The antimicrobial effects of the cements were measured with the agar diffusion test. A drop of material was directly applied into the plastic mold in a shape of a disk, which was created to ensure the standardized quantity of each material. Using molds, the error in the amount of material applied to microbial agar could affect false results. The disks of each material were prepared using approximately 10 mg of material. For each material, a new mold was used to prevent cross-contamination between materials. Disks were immediately placed on freshly inoculated plates with brain heart infusion (BHI) agar, using an aseptic technique in the aseptic chamber. Each plate contained negative control, which was represented by an empty paper disk in the middle of the agar plate.
Bacterial suspensions were prepared to a concentration of 0.5 MacFarland standard. BHI agar plates were inoculated with the respective bacterial strains, with a cotton swab, using an aseptic technique. The disk diffusion method of antimicrobial testing was used, and disks were placed onto the hardened BHI agar.
After inoculation, the agar plates were incubated at 37°C for 72 h under anaerobic conditions to allow sufficient growth of the bacteria. After incubation, the diameters of the zone of inhibition on microbial growth around each disk were measured in millimeters, using digital calipers.
STATISTICAL ANALYSIS:
Statistical analyses were performed using the software package SPSS version 21 (IBM Corp, Armonk, NY, USA). One-way ANOVA was used to assess differences between normally distributed mean diameters of zones of inhibition. The Kruskal-Wallis test was used when the data were not normally distributed. Statistical significance was set at
Results
Overall, 240 specimens were tested after being divided into 3 groups according to cement type. The effectiveness of each cement material is presented in Table 2 as mean inhibition zones in millimeters and accompanied standard deviations.
All tested cements showed antimicrobial effectiveness. Following that, different microorganisms were found to have reacted differently to different dental cement materials (
Pairwise comparisons showed that with Ketac cement there was no difference between
Statistically significant differences were observed among the different materials (
Discussion
We assessed 3 different commercial dental cements for their antimicrobial effectiveness against the 4 bacterial strains that most frequently create bacterial biofilm and lead to failure of cementation in fixed prosthodontics. The assessment was performed by the agar diffusion method, as this method was confirmed as appropriate for the determination of antimicrobial properties in other studies [21,26].
The retention of dental cements is often related to their properties and is determined by their resistance in the creation of bacterial biofilm and their avoidance of the creation of secondary caries [27–29]. Cements that have an antimicrobial effect can thus have a longer retention time of restorations. It is inevitable at some point that patients will develop early bacterial plaques, as the intraoral space of restoration between the cement and teeth is generally an ideal environment for bacterial growth [30].
The three dental materials tested were representative of glass ionomer cement (Ketac), zinc phosphate cement (Harvard FLB), and fluoride-releasing resin cement (Panavia SA Universal Dual Resin). Previous reports showed that glass ionomer cements have an antimicrobial effect, most likely due to their low pH or fluoride release [21–24]. There are also reports indicating that polycarboxylate cements and zinc phosphate cements have superior effects [23], which are also attributed to low pH. Our study showed similar results whereby resin cement showed the best antimicrobial effect, followed by zinc phosphate cement and glass ionomer cement. Here, it must be mentioned that all cements performed extremely well, showing superior zones of inhibition when compared with the negative control. This performance was observed with all 4 bacterial strains. Meanwhile, a study by Unosson et al [19] investigating the antimicrobial effects of different cements over time showed some antimicrobial effects at the beginning but no significant differences in the antibacterial effects for zinc phosphate cement when compared with the control in later time points. Also, the glass ionomer cement Ketac showed no difference when compared with the control. The reasons for these contradictory results could be the study methodology. In our study, we used the agar diffusion method, whereas Unosson et al [19] relied on measuring the viability through the direct contact test, based on the turbidimetric determination of continuous bacterial outgrowth from the material under investigation. Moreover, the time of evaluation also might play a crucial role. The agar diffusion method in the present study showed the antimicrobial effects 48 to 72 h after the incubation of bacteria, and in the other study, the authors evaluated the effect over a longer period.
Nevertheless, conventional cements create a low pH and therefore an acidic environment, which should limit the growth of microorganisms. However, with glass ionomer and zinc phosphate cements, low pH can cause pulpal irritation [31]. Moreover, a slightly acidic environment cannot inhibit the growth of bacteria. For instance,
Studies have shown that glass ionomers have antimicrobial properties against
Due to their ability to release zinc ions, zinc-containing materials can inhibit the growth of bacteria [38]. Zinc is an inhibitor of multiple activities in the bacterial cell in glycolysis, transmembrane proton translocation, and acid tolerance [41]. Its antimicrobial action is similar to the action of fluoride, but zinc works better in neutral pH (while the inhibitory potency of fluoride for glycolysis is much greater at acidic pH values). Zinc can also enhance proton permeability of bacterial cell membranes [41]. It reduces proton-extruding ATPase activity and ATP synthesis in glycolyzing cells because it can inhibit the glycolytic enzymes glyceraldehyde-3-phosphate dehydrogenases and pyruvate kinase, as well as the metabolism of phosphoenolpyruvate [42]. In our study, the activity of zinc was confirmed, and glass ionomer showed a bit less of the antimicrobial effectiveness, when compared with resin cement and zinc phosphate cement. However, fluoride release has been confirmed as an effective antibacterial agent also in other dental products [24]. Whether the effect was more related to creating an acidic environment or to fluoride release was not established in the present study. Regarding this matter, there are no established correlations between acidity or fluoride release and antibacterial properties. Rather, it has been proven that fluoride has a direct effect on the proliferation of bacteria, negatively affecting its growth [19]. Fluoride ions F− or HF directly inhibit the enzymes enolase, urease, phosphatases, and heme-catalase, which are involved in metabolism of bacterial cells. Moreover, HF is a transmembrane proton carrier and disturbs the membrane of the bacterial cell and overloads the proton-extruding ATPases, and eventually causes cell starvation [32].
In conclusion, the release of fluoride and zinc has an antimicrobial effect. It has been proposed that the ideal release from dental cements should be initially richer, then followed by a stable, lower release [36]. Of course, the releases might vary between different materials. We found that resin cement showed better antimicrobial effectiveness and has also been shown to have better, or at least a similar, release profile when compared with conventional glass ionomer cement [29,43,44].
Nevertheless, our study had limitations. The agar diffusion method that was used is semi-quantitative and depends on solubility and diffusion properties of the tested cement materials, so this might have impaired the results of material with lower solubility. In the present study, the performance of low pH, which also contributes to an antimicrobial effect, was not tested. It would be interesting to analyze the correlation between these 2 variables in the future. In addition, the levels of fluoride and zinc released might be of interest, as in the studies in the literature, there might be different levels of antimicrobial ability. Furthermore, this study was small and evaluated only 3 different materials. We encourage others to conduct additional studies and assess antimicrobial effectiveness of more agents within glass ionomer, zinc phosphate, and resin cements. Our study was conducted using in vitro conditions and could not simulate the physiological conditions of the oral cavity.
Conclusions
Antimicrobial properties in cement materials are desirable. Glass ionomer and resin cements released fluoride with a similar profile but showed slight differences in their performance of inhibition zones, which was most likely due to different levels of fluoride release. Meanwhile, zinc phosphate cement released zinc ions and also showed reliable antimicrobial ability in the inhibition of bacteria growth. Resin cements were statistically significantly better and might be applicable in clinical practice as the preferred dental cement material to reduce the probability of plaque formation and thus protect teeth from bacterial infections.
References
1. Hill EE, Dental cements for definitive luting: A review and practical clinical considerations: Dent Clin N Am, 2007; 51; 643-58
2. Sailer I, Fehér A, Filser F, Five-year clinical results of zirconia frameworks for posterior fixed partial dentures: Int J Prosthodont, 2007; 20; 383-88
3. Sbordone L, Bortolaia C, Oral microbial biofilms and plaque-related diseases: Microbial communities and their role in the shift from oral health to disease: Clin Oral Investig, 2003; 7; 181-88
4. Glantz P-OJ, Nilner K, Jendresen MD, Sundberg H, Quality of fixed prosthodontics after twenty-two years: Acta Odontol Scand, 2002; 60; 213-18
5. Uysal T, Ramoglu SI, Ertas H, Ulker M, Microleakage of orthodontic band cement at the cement-enamel and cement-band interfaces: Am J Orthod Dentofacial Orthop, 2010; 137(4); 534-39
6. Marsh PD, Controlling the oral biofilm with antimicrobials: J Dent, 2010; 38; S11-15
7. Korkmaz FM, Tüzüner T, Baygin O, Antibacterial activity, surface roughness, flexural strength, and solubility of conventional luting cements containing chlorhexidine diacetate/cetrimide mixtures: J Prosthet Dent, 2013; 110; 107-15
8. Magalhães APR, Moreira FCL, Alves DRS, Silver nanoparticles in resin luting cements: Antibacterial and physiochemical properties: J Clin Exp Dent, 2016; 8; e415-e22
9. Tüzüner T, Dimkov A, Nicholson JW, The effect of antimicrobial additives on the properties of dental glass-ionomer cements: A review: Acta Biomater Odontol Scand, 2019; 5; 9-21
10. Hook ER, Owen OJ, Bellis CA, Holder JA, Development of a novel antimicrobial-releasing glass ionomer cement functionalized with chlorhexidine hexametaphosphate nanoparticles: J Nanobiotechnology, 2014; 12; 3
11. Hamouda IM, Current perspectives of nanoparticles in medical and dental biomaterials: J Biomed Res, 2012; 26; 143-51
12. Gondim BLC, Castellano LRC, de Castro RD, Effect of chitosan nanoparticles on the inhibition of Candida spp. biofilm on denture base surface: Arch Oral Biol, 2018; 94; 99-107
13. Paiva L, Fidalgo TKS, da Costa LP, Antibacterial properties and compressive strength of new one-step preparation silver nanoparticles in glass ionomer cements (NanoAg-GIC): J Dent, 2018; 69; 102-9
14. Ibrahim MA, Neo J, Esguerra RJ, Fawzy AS, Characterization of antibacterial and adhesion properties of chitosan-modified glass ionomer cement: J Biomater Appl, 2015; 30; 409-19
15. Millett DT, Duff S, Morrison L, In vitro comparison of orthodontic band cements: Am J Orthod Dentofacial Orthop, 2003; 123(1); 15-20
16. Prabhakar AR, Mahantesh T, Ahuja V, Comparison of retention and demineralization inhibition potential of adhesive banding cements in primary teeth: J Dent Child, 2010; 77(2); 66-71
17. Cantekin K, Delikan E, Cetin S, In vitro bond strength and fatigue stress test evaluation of different adhesive cements used for fixed space maintainer cementation: Eur J Dent, 2014; 8(3); 314-19
18. Aggarwal M, Foley TF, Rix D, A comparison of shear peel band strengths of 5 orthodontic cements: Angle Orthod, 2000; 70(4); 308-16
19. Unosson E, Cai Y, Jiang X, Antibacterial properties of dental luting agents: Potential to hinder the development of secondary caries: Int J Dent, 2012; 2012; 529495
20. Featherstone JD, Prevention and reversal of dental caries: role of low level fluoride: Community Dent Oral Epidemiol, 1999; 27(1); 31-40
21. Vermeersch G, Leloup G, Delmee M, Vreven J, Anti-bacterial activity of glass-ionomer cements, compomers and resin composites: Relationship between acidity and material setting phase: J Oral Rehabil, 2005; 32(5); 386-74
22. Matalon S, Slutzky H, Weiss EI, Antibacterial properties of 4 orthodontic cements: Am J Orthod Dentofacial Orthop, 2005; 127(1); 56-63
23. Lewinstein I, Matalon S, Slutzkey S, Weiss EiI, Antibacterial properties of aged dental cements evaluated by direct-contact and agar diffusion tests: J Prosthet Dent, 2005; 93(4); 364-71
24. Wiegand A, Buchalla W, Attin T, Review on fluoride-releasing restorative materials – fluoride release and uptake characteristics, antibacterial activity and influence on caries formation: Dent Mater, 2007; 23(3); 343-62
25. Papagiannoulis L, Kakaboura A, Eliades G, In vivo vs in vitro anticariogenic behavior of glass-ionomer and resin composite restorative materials: Dent Mater, 2002; 18(8); 561-69
26. Imazato S, Antibacterial properties of resin composites and dentin bonding systems: Dent Mater, 2003; 19(6); 449-57
27. Libby G, Arcuri MR, LaVelle WE, Hebl L, Longevity of fixed partial dentures: J Prosthet Dent, 1997; 78(2); 127-31
28. Goodacre CJ, Bernal G, Rungcharassaeng K, Kan JYK, Clinical complications in fixed prosthodontics: J Prosthet Dent, 2003; 90(1); 31-41
29. Montanaro L, Campoccia D, Rizzi S, Evaluation of bacterial adhesion of Streptococcus mutans on dental restorative materials: Biomaterials, 2004; 25(18); 4457-63
30. Hannig M, Transmission electron microscopy of early plaque formation on dental materials in vivo: Eur J Oral Sci, 1999; 107(1); 55-64
31. Hiraishi N, Kitasako Y, Nikaido T, Acidity of conventional luting cements and their diffusion through bovine dentine: Int Endod J, 2003; 36(9); 622-28
32. Marquis RE, Clock SA, Mota-Meira M, Fluoride and organic weak acids as modulators of microbial physiology: FEMS Microbiol Rev, 2003; 26(5); 493-510
33. Castilho ARF, Duque C, Kreling PF, Doxycycline-containing glass ionomer cement for arresting residual caries: An in vitro study and a pilot trial: J Appl Oral Sci, 2018; 26; e20170116
34. Cury JA, Oliveira BH, Santos APP, Tenuta LMA, Are fluoride releasing dental materials clinically effective on caries control?: Dent Mater, 2016; 32; 323-33
35. Hahnel S, Ionescu AC, Cazzaniga G, Biofilm formation and release of fluoride from dental restorative materials in relation to their surface properties: J Dent, 2017; 60; 14-24
36. Dastjerdie EV, Oskoui M, Sayanjali E, Tabatabaei FS, In-vitro comparison of the antimicrobial properties of glass ionomer cements with zinc phosphate cements: Iran J Pharm Res, 2012; 11(1); 77-82
37. Hiraishi N, Kitasako Y, Nikaido T, Acidity of conventional luting cements and their diffusion through bovine dentine: Int Endod J, 2003; 36; 622-28
38. Boyd D, Li H, Tanner D, The antibacterial effects of zinc ion migration from zinc-based glass polyalkenoate cements: J Mater Sci Mater Med, 2006; 17; 489-94
39. Osinaga P, Grande R, Ballester R, Zinc sulfate addition to glass-ionomer-based cements: Influence on physical and antibacterial properties, zinc and fluoride release: Dent Mater, 2003; 19; 212-17
40. Vermeersch G, Leloup G, Delmee M, Vreven J, Antibacterial activity of glass – ionomer cements, compomers and resin composites: Relationship between acidity and material setting phase: J Oral Rehabil, 2005; 32; 368-74
41. Phan T-N, Buckner T, Sheng J, Physiologic actions of zinc related to inhibition of acid and alkali production by oral streptococci in suspensions and biofilms: Oral Microbiol Immunol, 2004; 19; 31-38
42. Daugela P, Oziunas R, Zekonis G, Antibacterial potential of contemporary dental luting cements: Stomatologija, 2008; 10(1); 16-21
43. Forsten L, Fluoride release and uptake by glass-ionomers and related materials and its clinical effect: Biomaterials, 1998; 19(6); 503-8
44. Yoshida K, Atsuta M, Properties of fluoride-releasing light-activated resin cement: Dent Mater, 1999; 15(5); 337-41
Tables
 Table 1. Distribution of samples according to the testing groups.
Table 1. Distribution of samples according to the testing groups. Table 2. Mean zones of inhibition (diameter in mm) ± standard deviation for respective cement material according to the disk diffusion method.Table 1. Distribution of samples according to the testing groups.Table 2. Mean zones of inhibition (diameter in mm) ± standard deviation for respective cement material according to the disk diffusion method.
Table 2. Mean zones of inhibition (diameter in mm) ± standard deviation for respective cement material according to the disk diffusion method.Table 1. Distribution of samples according to the testing groups.Table 2. Mean zones of inhibition (diameter in mm) ± standard deviation for respective cement material according to the disk diffusion method. Most Viewed Current Articles
13 Apr 2020 : Original article 22,472
Outcome of 24 Weeks of Combined Schroth and Pilates Exercises on Cobb Angle, Angle of Trunk Rotation, Chest...DOI :10.12659/MSMBR.920449
Med Sci Monit Basic Res 2020; 26:e920449
20 Apr 2018 : Original article 19,981
Brain Training Games Enhance Cognitive Function in Healthy SubjectsDOI :10.12659/MSMBR.909022
Med Sci Monit Basic Res 2018; 24:63-69
23 Jul 2016 : Review article 12,261
Cardiac Hypertrophy: An Introduction to Molecular and Cellular BasisDOI :10.12659/MSMBR.900437
Med Sci Monit Basic Res 2016; 22:75-79
26 Sep 2024 : Original article 11,848
Methods of Processing Dental Chromium-Cobalt Alloys for Production of Metal Frameworks Faced with Ceramics ...DOI :10.12659/MSMBR.944051
Med Sci Monit Basic Res 2024; 30:e944051